It’s an exciting time in the world of femtech with multiple products being developed for taking our overnight temperature.
Oura Ring is a new player in fertility awareness. Oura Ring partnered with Natural Cycles, a temperature-only (with optional LH) fertility awareness based method. As of 2022, the ring is approved for use with syncing with Natural Cycles.
Get the sizing kit and don’t make my mistake of ordering the ring size you usually wear 😂
As a traditional charter of my cycle, I wanted to see if Oura Ring would be a good fit as a cross-check to help confirm ovulation without syncing to Natural Cycles.
After five cycles of use and comparisons to other thermometers, I am confident in saying that Oura Ring can be used as sympto-thermal method cross check with some tweaking and conversions. Read on if you would like to see examples and my method of conversion in order to avoid paying that extra fee to Natural Cycles.
If you are charting to avoid pregnancy and reading this article, I highly recommend cross-checking with cervical mucus, cervical position, and/or urinary hormones in addition to the Ring. I do NOT recommend using the Ring alone to avoid pregnancy. If you are seriously avoiding, you should use at least one of the signs mentioned above and wait until those rules are met before having unprotected sex. You should cross-check with oral or vaginal temperatures for a minimum of 2-3 cycles before relying on Oura to confirm ovulation.
Wejust don’t have the kind of evidence necessary for me to recommend using Oura without other fertility signs, particularly for those strictly avoiding a pregnancy. If you are charting to conceive, then this Ring is perfectly acceptable for confirming you are in your luteal phase.
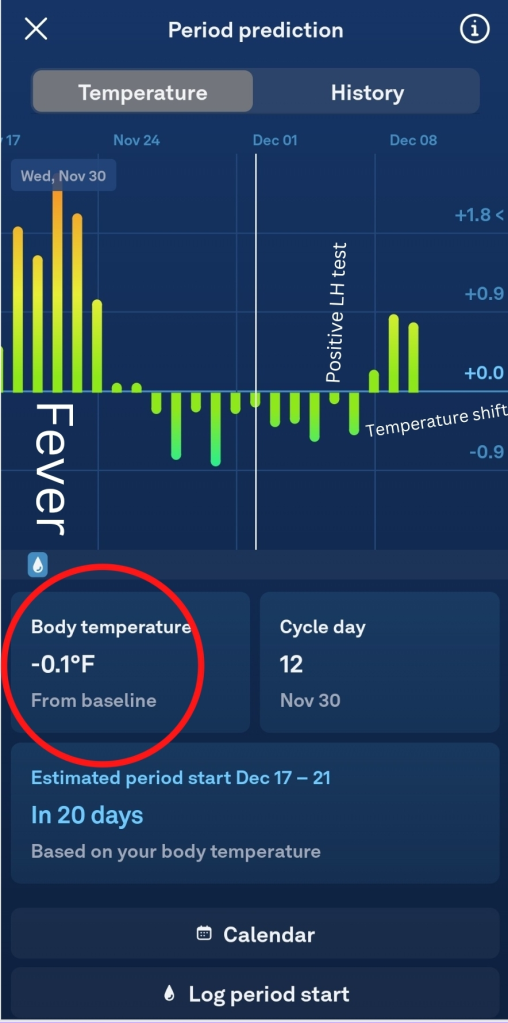
VIEW FROM THE OURA RING PERIOD PREDICTION SCREEN. OURA will predict menstruation based on body temperature and cycle dates.
Oura Ring is worn 24/7 for full use of its features. Overnight, it detects your sleep and a temperature is determined at this time. Your temperature is displayed when you sync Oura to the app in the morning as a +/- deviation from baseline, as shown in the photo above.
To chart your temperature in an app without Natural Cycles, you will need to choose a baseline. Remember, when we are charting our cycles, we are pattern making. You will need to translate the deviation to the chart so that you can see a pattern of lower and higher temperatures. I chose 97 degrees Fahrenheit as my baseline because it is a whole number that falls in the middle of most fertility awareness charts.
On Day 17, my deviation was -.6 F on Oura. I subtracted -.6F from 97F and got 96.4. That is the temperature I then chart. On Day 18, my deviation was +.3F on Oura. I added .3F to 97F and charted 97.3F on my chart. This formula allows me to see the pattern on a standard chart from Read Your Body.
Traditional methods call for two decimal points. However, this isn’t necessary to see a pattern with ring temperature. Finger temperature tends to show larger temperature shifts than standard waking body temperature taken at the mouth.
If you want to see two decimal places, you must initially purchase a subscription with Natural Cycles.
The official statement from Oura is that you shouldn’t compare it to other thermometers or use it without Natural Cycles. The reason they say not to compare it is because all thermometers will give different results. As charters, we are smart enough to know that we are looking for patterns and not the exact same result. The reason that they say to use it with Natural Cycles is likely because of the paid partnership as well as to avoid liability for unintended pregnancies. I’d like to say again that using Oura for a traditional FAM without Natural Cycles only has case study level evidence and is not currently endorsed by any organizations. Consider this when choosing it!
Two decimal plays after syncing with Natural Cycles.
What else does Oura ring do that can help me track my cycle health?
Sleep information (quality, amount, phases, disturbance)
Steps, exercise, calories
Meditation and winding down for sleep
Stress levels, illness
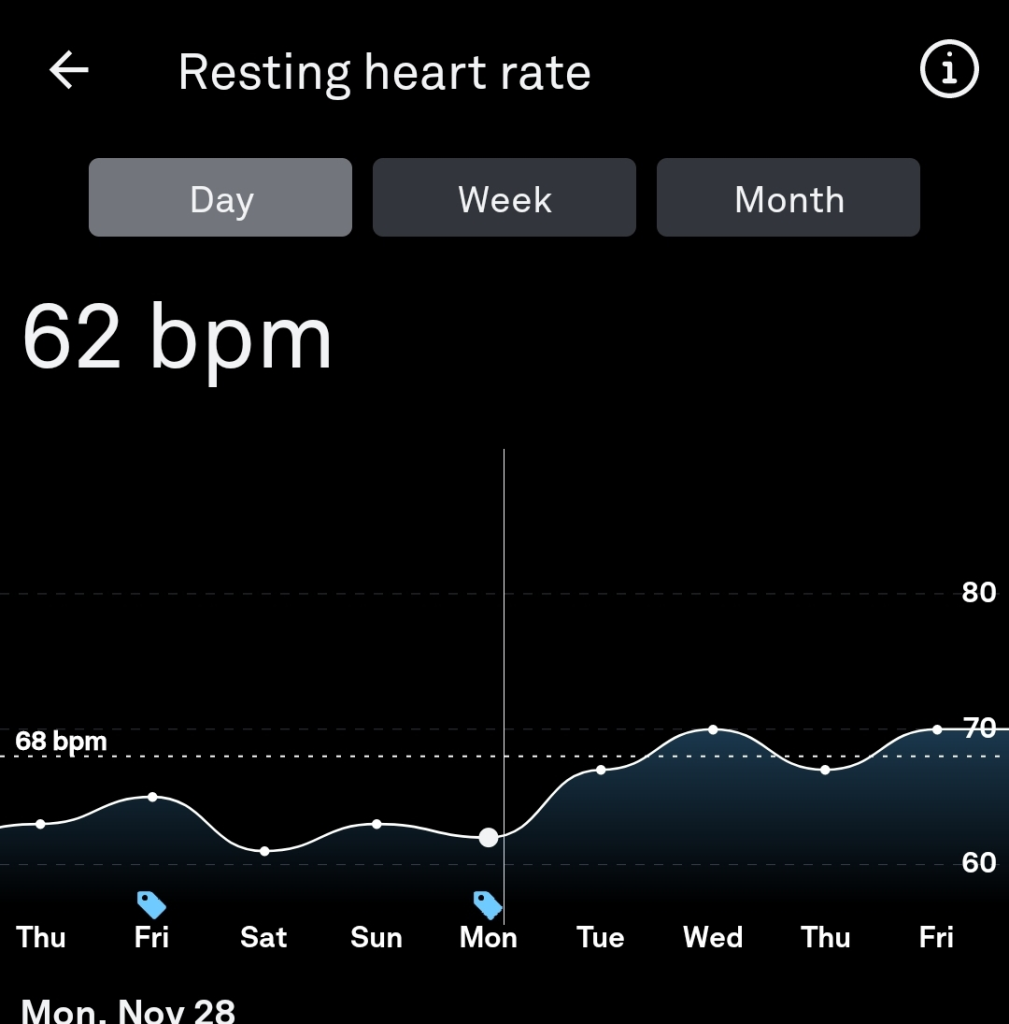
Resting heart rate and sleeping heart rate
Rest mode feature. If you have painful periods or are debilitated by any illness, Oura can be informed that you are sick or unwell and your statistics on it will change.
Resting heart rate changes with the phases of the cycle, rising in the fertile window and then again after ovulation. This can be a useful extra sign for cycle tracking. Read my other article on RHR.
What are the details?
It is initially approximately $300 USD depending on the model and time of year.
It is free to the use the app for the first 6 months, and then it is $5.99 USD per month. I’ve heard some people say they have used without subscribing, but can’t say if temperature feature is available without paying.
The battery life is about 5-7 days with all day use and takes about 30 minutes to fully charge.
You can use my link for $50 USD off. This link only works for five people. I will periodically replace the link once a new one becomes available.
For me, the greatest selling point for this ring is NEVER having to remember taking your temperature again. I’m an adult with a busy life and this makes charting so much easier for me. I charge my ring once a week and otherwise forget about it. This is definitely my current favorite femtech for charting your cycle.
It’s somewhat embarrassing to admit, but I find it hard to bring fertility awareness up to people in real life who haven’t heard of it before. For me, the awkwardness is their reaction to the name and what they think it entails.
Something about “fertility awareness” evokes something for some folks that is akin to “hippy” or “new age” type of connotations.
On the other end, some folks will think that this term means the calendar method or the rhythm method. This is partially because most people don’t know about the new science of real-time fertility signs. The other reason people think this is because most people who claim to be practicing a fertility awareness method are still doing some kind of bleeding tracking focused method. It’s truly a small percentage of us who are using a evidence-based real-time fertility sign method like Sympto-Hormonal, Sympto-Thermal, or Cervical Mucus only methods.
“Fertility” evokes conception for many folks. It also isn’t the correct word. We can only know if we were truly capable of fertility that cycle retrospectively when a pregnancy occurs, or if the cycle was visibly fertile by counting the luteal phase. I’ve seen a researcher say the correct term might be “fecundity.”
“Awareness” makes me think of some type of campaign. And what does awareness mean?According to the OED, “knowledge or perception of a situation or fact.” This can sound like people are charting with their intuition, but we are not. Fertility awareness modern methods track tangible and measurable fertility signs (cervical mucus, basal body temperature, cervix) or hormone levels.
I also don’t want to tell people that I teach natural family planning. Something about “family planning” makes people assume that the method is only for those who want to conceive, but a part of family planning is avoiding a pregnancy too. Then, there’s the religious connotation. I’m not Catholic, and I don’t just encourage abstinence because of religious compulsion.
Then, there’s the word natural. Natural is an incredibly subjective term. Some folks will see it and think this also means the withdrawal or pull out method. In the context of charting, it does not include withdrawal. According to the OED, one of natural’s meanings is “existing in or caused by nature; not made or caused by humankind.”
With this definition, do urinary hormones methods become “unnatural”? The hormones themselves occur in the human body, but you can only measure them with help from a machine. I’m not arguing against natural family planning including hormone monitors, but I do wonder if it makes sense to use that terminology.
My favorite terminology is “fertility awareness based methods.” Something about the word “based” makes it sound more scientific in my mind. I’ve seen some educators adopt this language to be more inclusive.
I’ve seen Samantha Zipporah talk about “conscious contraception” as a way to classify fertility awareness. I like the term conscious. Something about it sounds more sophisticated than awareness. I’ve seen it used in a few older academic articles. You can read them here and here.
I’ve also seen it called “Natural Fertility Control” or “NFC.” You can read an article with this terminology here. Some people will feel uncomfortable with the term “control.” In some ways, it isn’t control, because there is always a small chance of unintended pregnancy with correct use, and a larger chance of unintended pregnancy with incorrect use. I do think the self-knowledge gives the user a level of control over their choices more than other methods do. After all, with correct use, you will always know when you are possibly fertile, and then can make your decisions accordingly.
Many people think that having sex during menstruation cannot lead to pregnancy, but the answer is much more nuanced than that. It is possible to get pregnant during bleeding episodes, some of which may not be menstruation!
Was the bleeding truly menstruation?
Charting evidence-based fertility signs like cervical mucus, basal body temperature, and urinary tests are the best way to determine if you are ovulating. True menstruation should follow about 10-16 days post ovulation as indicated by a temperature shift or positive PdG test.
If you are not charting your cycle with a fertility awareness based method, your bleeding may not really be menstruation. Estrogen breakthrough bleeding may appear very similar to menstruation and is often indistinguishable without charting. This bleeding can be fertile, and pregnancy could result.
Day one of a true menstruation marks the beginning of the cycle.
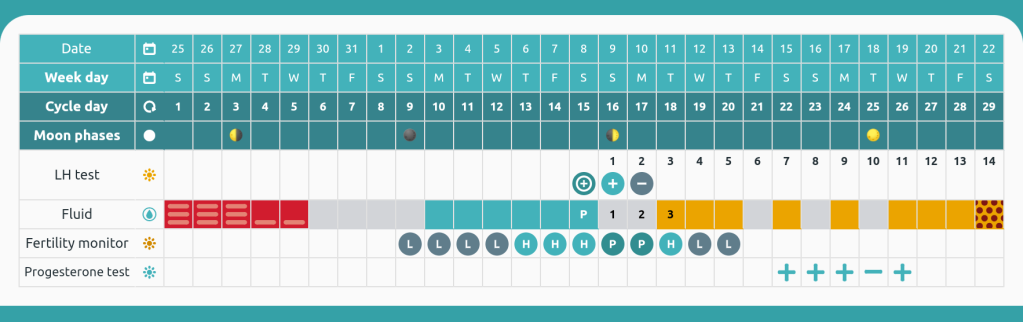
Day 1 is true menstruation because it followed a proven luteal phase. The current cycle confirms the next bleed will be menstruation because of the positive progesterone tests. This app is Read Your Body.
How long are your cycles? Better yet, approximately when do you usually ovulate?
If your cycles were 26 days or longer for the last year, it is unlikely you will become pregnant with sex during the first five days of the cycle.
Dr. Josef Roetzer monitored 5,807 cycles. He observed only one pregnancy before day 6 of the cycle. Her cycles were 22-27 days long.
Dr. Roetzer estimates that using the first five/six days is 99.8% effective for avoiding pregnancy. It is important to note that all of his cycles monitored had a temperature shift preceding menstruation. If you do not have proof that you ovulated before a bleed, it becomes more likely to conceive during bleeding.
Another way to determine the last infertile day at the beginning of the cycle is to use Dr. Doering’s rule. Dr. Doering subtracted 7 from the earliest first high temperature in the last year. For example, Sarah’s earliest first high temperature was day 13. Day 13 – 7 = Day 6 as the last infertile day of the cycle. This rule is always crosschecked with cervical mucus. Sperm may survive up to 5 days in cervical mucus, and any presence that has not been determined to be infertile through instruction should open the fertile window. The Doering rule is more personalized than automatically assuming the first five/six days are infertile.
In Dr. Frank-Hermann’s double-check sympto-thermal study from 2007, all three method failures were from day 5 intercourse. This study used the first five day rule and Doering rule. This study yielded an efficacy of 99.6%.
So am I safe to have sex during my period? Ask yourself these questions.
Did you confirm ovulation with basal body temperature, PdG strips, or a blood draw in the previous cycle?
Are your cycles longer than 26 days on average? Have you ever had a peak day before day 13 of the cycle?
If the answer to both of those is yes, you can probably have safe sex up to day 5 of your cycle.
If your answer is no, then you have a possibility of pregnancy.
What if I want to be more conservative?
Some methods like Billings, FEMM, and Creighton suggest not having sex during heavy days of bleeding when cervical mucus cannot be observed.
If you have a history of short cycles (less than 26 days) or want to add an extra layer of protection onto the beginning of the cycle, I recommend beginning observing vulva sensation and cervical mucus as soon as your bleeding has lightened enough to no longer need a tampon, cup, or regular pad. If you need only a panty liner or are only experiencing light spotting, you should beginning checking your cervical mucus and sensation throughout the day. At the end of your day, if you have observed no cervical mucus or sensation outside of your determined infertile pattern, this day is safe for sex. (DO NOT DO THIS WITHOUT LEARNING A METHOD. THIS BLOG IS NOT ENOUGH INFORMATION TO AVOID PREGNANCY WITH ALONE).
What if I bleed for more than 5 days?
If your menstruation lasts longer than five days, you should follow the instructions from the paragraph above. It is NOT safe to consider past day 5 automatically available if you are bleeding. You need proof by using cervical mucus or urinary estrogen tests that your fertile window has not yet opened past day 5 of the cycle.
What if I randomly have a short cycle?
Checking cervical mucus is your best back up. Cervical mucus should appear when the fertile window is opening for most charters. Many methods suggest no longer considering menstruation safe once you enter peri-menopause (can occur up to 10 years before menopause) because cycles may shorten at this time. If you notice that your cycles have grown shorter than 26 days, you may want to become more vigilant and stop automatically considering the first 5 days safe.
Conclusion
For the majority of people menstruating, using the first five days of a true menstrual cycle will not result in pregnancy. For a very small percentage, it may. I recommend charting with a real fertility awareness method (Sensiplan, SymptoPro, FEMM, Billings, Marquette, etc) to determine if your bleeding is actually menstruation!
Works Cited
Roetzer, Josef. “Further Evolution of the Sympto-Thermal Methods.” International Review of Natural Family Planning 1 (1977): 139-150.
During the postpartum period of time, fertility is in a unique state. For those fully breastfeeding, it may be months or years before they begin ovulating again regularly and with fertile cycles. This article talks about some of the data we have on what return of fertility looks like. This information may be of particular interest to those charting with a method of natural family planning or fertility awareness. Charting at this time may be difficult, and for highest efficacy should be done closely with a certified natural family planning educator.
Breastfeeding as Birth Control
Breastfeeding has been shown over numerous studies to have an effect on return to fertility and ovulation. Kennedy et al (1989) reviewed 10 studies from multiple countries to come to a consensus on what full-breastfeeding means.
Fully breastfeeding or at least partially fully breastfeeding
Fully breastfeeding meaning the infant gets all or as close to all as possible of their nutrition by suckling at the breast directly, no bottles or pumping
Small bites of regular food or water do not disqualify for full breastfeeding
No bleeding past day 56 postpartum until the 6 month mark postpartum.
Some methods suggest going no longer than 6 hours at night without breastfeeding. While this was not mentioned in the study, it is generally used as the standard in fertility awareness based methods to see if someone qualifies to rely on the lactational amenorrhea method (LAM).
LAM is 98% effective for avoiding pregnancy when all criteria is met up until 6 months postpartum. After that, efficacy drops precipitously.
What about ecological breastfeeding?
Ecological breastfeeding requires even stricter criteria and may delay fertility for much longer. Bleeding past day 56 does not disqualify someone for ecological breastfeeding. Ecological breastfeeding should not be confused with LAM! Ecological breastfeeding was coined by Dr. Sheila Kippley. You can buy her book here.
The criteria include:
Breastfeed exclusively for 6 months
Pacify your baby at your breast
No bottles or pacifiers
Sleep with your baby for night feedings
Sleep with your baby for a daily-nap feeding
Nurse frequently day & night. Avoid schedules.
Avoid anything that would separate you from your baby / prevent regular nursing
Symptothermal Method Studies on Breastfeeding
For the first part of this overview, I am going to cover a few symptothermal studies that followed breastfeeders from birth to return of fertility. Symptothermal charters record cervical mucus and basal body temperature daily in order to track their fertility and determine when the fertile window is opened and when it is closed.
In “Breastfeeding and the Symptothermal Method,” Kennedy et al. followed 73 women who charted with a symptothermal method in Australia, Canada, England. While this is a small sample size, the team collected a ton of data: 22,538 diary sheets, 9,428 urinary vials to measure hormones, and 1,600 follow-ups with the women (Kennedy 1995).
Kennedy et al. reported the following data regarding the wait to return of fertility:
Only 25% of first ovulations postpartum had “adequate luteinization.” This means over three quarters of first ovulations were likely infertile (Kennedy, 110).
In retrospect, up to 51% of possibly fertile days identified by sympto-thermal would not have lead to conception (Kennedy, 112). The study standard for this was 5 day sperm life.
They found that 94-99% of the time, the sympto-thermal method correctly identified when a day was really infertile. This means that around 1-6% of the time it didn’t identify a day that may have lead to pregnancy (Kennedy, 112).
They recorded four adequate ovulations with those fully breastfeeding for their first ovulation. This was defined as a 10 day or greater luteal phase with adequate progesterone levels. (Kennedy, 112).
Abstinence was expected per the rules for about 50% of the charted days included in the study (Kennedy, 113).
Bonus Information for Cervical Mucus Fans: Fertile mucus in this study was considered anything cloudy, opague, clear, translucent, stretchy, strands, wet, lubricative, moist, or unusually abundant.
Zinaman and Stevenson in the USA followed 25 women until they had 3 ovulatory cycles postpartum (1991).
They found the following data regarding return to fertility:
20% of ovulations in the first ovulation postpartum during the first 6 months were considered fertile (ie a luteal phase longer than 10 days) (Zinaman and Stevenson, 2037).
Basal body temperature appeared inadequate to capture the first ovulation, occurring up to 4 days after the LH peak, but it improved in later cycles (Zinaman and Stevenson, 2037).
Percentage
Time to Return of Fertility From Birth
25%
Less than 200 days
25%
200 to 300 days
35%
301 to 400 days
15%
More than 400 days
Time to return of fertility among 25 breastfeeding women in Washington, DC. Created from page 2037 in Zinaman and Steveson (1991).
Parentau-Carreau reports the following data on postpartum charting:
65% of first bleeds were preceded by a thermal shift (35).
The collection of charts confirmed the theory that 4 high temperatures should be used postpartum, as there were instances of 3 raised temperatures that were not true shifts (36).
Among temperature shifts during the first 6 months postpartum, 75% lasted 8 days or more (37).
For babies who sucked their thumb or used a pacifier regularly, their mothers experienced return of fertility an average of 13 days earlier than those who only breastfed for soothing purposes (37).
The basal body temperature curve tended to become more steady or regular in the one to two weeks prior to the first ovulation (38).
What can we conclude from all this data?
Breastfeeding and meeting the criteria for LAM is highly effective for avoiding pregnancy in the first 6 months postpartum.
Most first ovulations postpartum are infertile (defined as a luteal phase less than 10 days long).
It is possible to chart during postpartum to avoid pregnancy.
What methods work best postpartum?
I recommend practicing either the Billings Ovulation Method or Marquette postpartum. I do not recommend sympto-thermal method because temperatures are not useful until fertility returns. I only recommend taking your temperature before the 6 month mark to those who are not breastfeeding. In addition, the sympto-thermal method offers less complex mucus patterns than Billings does.
Billings Ovulation Method involves charting sensation at the vulva and appearance of mucus to create a basic infertile pattern. It allows only alternate evenings of the basic infertile pattern for sex until return of fertility (IE ovulation) occurs. It is approximately 98% effective with correct use postpartum.
Subjective fertility signs (sensation and appearance)
Only alternate evenings for sex
Very affordable (Billings will work to set you up with a free instructor if you absolutely cannot afford one)
No re-occurring cost
One-time cost for instruction (ideally, please pay your educator if you can! Some instructors may charge after 1-2 years pass)
Marquette Method involves charting urinary hormones using the Clearblue monitor. This monitor reads estrogen and LH levels. This method is going to be more expensive than a cervical mucus only method, so I only recommend it to those who can afford approximately $30 USD a month or more postpartum. Unfortunately, the stick costs fluctuate up to $50 USD or so for 30 sticks, but I have seen them as low as $30 USD. Marquette is approximately 98% effective with correct use.
Objective fertility signs (monitor does the reading for you)
Any time of day sex when available
Expensive by some standards. Sticks cost twice as much in Europe. May not be available in some countries at all.
Re-occurring cost
One-time cost of the monitor ($50-$130 USD depending on if buying new or used)
One-time cost of instruction (unless you go over the year mark, you may need to pay twice)
I have heard that some instructors may offer scholarships, but you would need to contact individual instructors or organizations to learn their policies.
References
Kennedy, K; Rivera, R; McNeilly, A. (1989). Consensus statement on the use of breastfeeding as a family planning method. , 39(5), 0–496. doi:10.1016/0010-7824(89)90103-0
Kennedy, K., Gross, B., Parenteau-Carreau, S., Flynn, A., Brown, J., & Visness, C. (1995). “Breastfeeding and the Symptothermal Method.” Studies in Family Planning,26(2), 107-115. doi:10.2307/2137936
Parenteau-Carreau, S. (1984). “The Return of Fertility in Breastfeeding Women.” The International Review of Natural Family Planning. Vol. 8(1). pp. 34-38.
Zinaman, Michael; Stevenson, Wilma (1991). Efficacy of the symptothermal method of natural family planning in lactating women after the return of menses. American Journal of Obstetrics and Gynecology, 165(6), 2037–2039. doi:10.1016/S0002-9378(11)90575-4
I began this certification having been quite dissatisfied with my previous certification in the sympto-thermal method. I found the sympto-thermal method inadequate for irregular cycles or postpartum cycles, as well as for any cycles with continous mucus.
This certification 100% cleared up all doubts I had about being able to teach people in these situations! I love that Billing’s motto is “Keep it simple.” Ultimately, this certification gave me the confidence to give up temperature taking as a part of my fertility awareness routine.
First Step:
Before beginning the certification, I took an introductory class with my spouse in the method. This gave me about 6 months to try to apply the principles to my charts before beginning training. I had previously certified in a “Billings-based method” but learned quickly that authentic Billings is a different creature altogether.
I recommend that anyone who is going to train in this method learn to practice it first for at least 6 to 12 cycles under the guidance of an accredited teacher. Joining this program without learning the method first is going to leave you lost on your charts – when you should be confident in your charts before helping others.
Second Step:
The class began in December 2019 and ran through September 2020. We met once a month for approximately an hour (sometimes a little more or less). Inbetween meetings, we were expected to read one to two chapters of material and complete 5 or more worksheets that included chart evaluation and quizzes.
I really appreciated the live classes because my previous certification had no live component. I’m a strong believer that synchronous connection is really important for learning something new.
During class, we were shown PowerPoints and given time to ask questions about the homework. Hearing from long-term accredited teachers about different charting circumstances did wonders for my existing knowledge base. It was incredibly valuable.
Full disclosure: It is important to know that Billings was founded by and is primarily run by Catholics. These meetings often began with prayer or referenced God. Teachers are not required to teach the religious component of the PowerPoint. That means that Billings can be presented in a secular manner. The WOOMB International head organization notably does not include religious elements in their presentation of the method. The science of the method is solid regardless of any ideology attached to it.
Third Step:
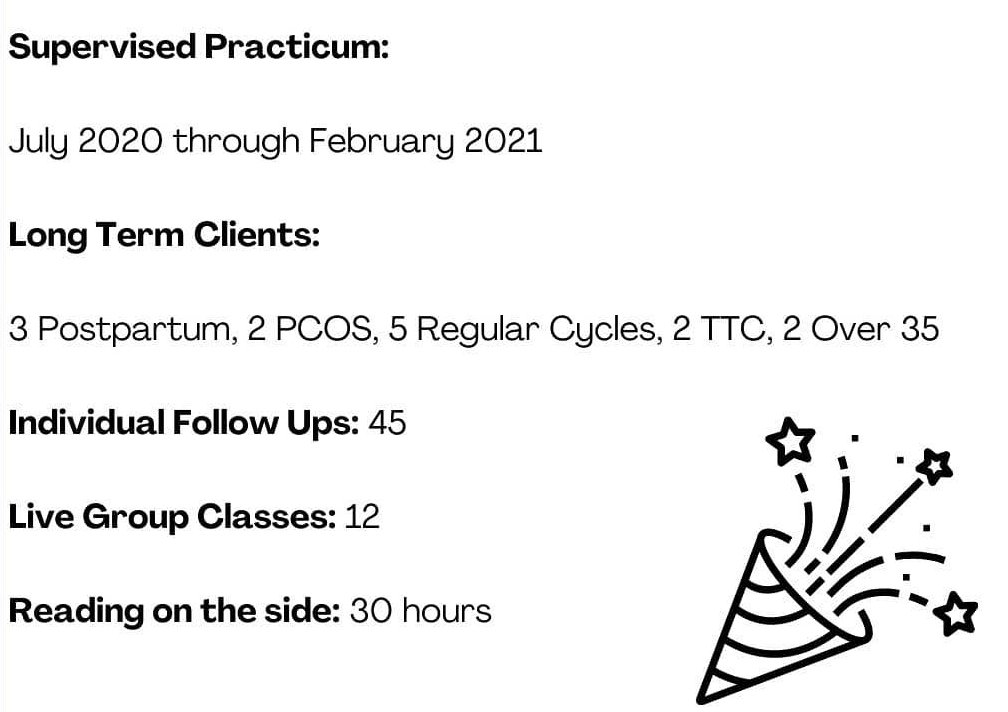
The next step after passing an exam on the material was to begin practicum. Practicum is the supervised portion of the certification where you teach 6 to 10 clients minimum in the method while submitting charts and questios to a supervisor selected for you by the organization.
This graphic is how long it took me to finish the practicum portion of the course. Most people take 1.5 to 2 years to finish the program. I went a little faster because I taught larger group classes and had clients lined up before it began.
Practicum was the most enriching part of the experience, and I recommend that anyone who does the training utilize this time to your best advantage. I learned how to help people identify complex basic infertile patterns where they never have dry days. This was not possible in my previous method. I was able to support multiple postpartum women as well as folks with PCOS or who were trying to conceive. I learned so much by meeting with my clients and sending charts to my supervisor.
The follow-ups and classes in Billings are mandatory live meetings (video calling, phone call, or in-person). The follow-ups generally last 15 to 30 minutes depending on the client and how early they are in the process. Follow-ups and classes are required to be live, and this is based on what was done to reach efficacy in the Billings studies. We generally meet with clients seven or more times in the first 6 months, and then every 1 to 3 months. Some people may have more or less follow-ups depending on when they reach autonomy and things like cycle characteristics (postpartum people tend to meet up until the third ovulatory cycle after return of fertility.)
Fourth step:
After having enough clients in different situations (postpartum, trying to conceive, trying to avoid, regular and irregular cycles), I had a final meeting with my supervisor. Before this, I had to compile a document of every client chart. This was a bit laborious as the Billings charts cannot be exported to PDF without losing part of the chart. I had to screenshot segments of the charts and then re-assemble them. This meeting with my supervisor lasted about two hours, and we discussed all of my client charts and any corrections that needed to be made.
Following that, I was recommended for the final step. I recieved a mailed in exam that involved correcting a full paper chart and writing why I made those changes and what mistakes were originally made.
I turned in this exam to two graders. They then met with me and discussed the chart and any necessary corrections. They approved my certification at the end of the meeting.
The Future
Billings Ovulation Method teachers are required to do continuing education to maintain their certification. This is an investment of approximately $300 to $600 every three years. While this is costly, it is really important to attend further training where the teacher can see more advanced charting techniques and learn about health conditions, efficacy, and more!
My Final Thoughts
I would recommend this certification program to anyone who is interested in having an in-depth understanding of cervical mucus charting. The Billings Method teaches about things like the “pockets of shaw” and the cervical mucus crypts. My previous certification did not include close study of the patterns of cervical mucus. This program fundamentally changed my thinking about temperatures always being a necessary part of charting. I ended up dropping temperatures completely after 3 years of using basal body temperature.
Billings allows teachers to order all supplies, including digital materials, for clients. This means I do not have to produce my own materials, and it is super useful for quickly mailing clients what they need.
To make the most of out of this program, I recommend also reading the scientific studies on the side. Unfortunately, the program did not go into a lot of depth on the previous research studies. As someone in academia, I really like understanding all the different correct use and typical use statistics. I’m often questioned about efficacy, and I want to be able to answer people’s questions. If this also describes you, I recommend the following articles:
This article is for the husbands, boyfriends, spouses, or sexual partners of anyone using a form of fertility awareness for pregnancy prevention.
Charting cycles for pregnancy prevention is a big life change, especially for the female charter. While the charter has to learn to interpret their cycles, it is fundamental that they have a supportive partner in the process.
So, What is Fertility Awareness?
Fertility awareness involves tracking one or more bio-markers of the female cycle. These bio-markers include: cervical mucus, basal body temperature, cervical position, urinary hormones, and cycle start dates. The bio-markers are used to draw a fertile window. Fertility awareness has been studied scientifically for nearly a hundred years. There are a plethora of studies on the topic. Click here to read the 2018 Overview of FABMs. In general, you can expect approximately 98 to 99% efficacy across all modern fertility awareness methods.
Your partner will be tracking based on whatever method she chooses. A method is a way of categorizing bio-markers. For example, I teach the Billings Ovulation Method. This method tracks the bio-marker cervical mucus along with sensation felt at the vulva.
One of the first things you will learn when charting is that MALES ARE FERTILE 24/7. Females are fertile only cyclically, and on average the fertile window will be for less than 1/3rd of the female menstrual cycle.
In the beginning, there is sometimes a steep learning curve with tracking these signs. Your partner may forget to check cervical mucus at every restroom break or they may be erratic in taking their temperatures. Your role at this time is be supportive. If you are living with your partner, you can help remind her to take her temperature upon first waking (if they are choosing to chart this sign!) You may also want to take part in keeping the chart.
While it is relatively rare for the partner to help chart, it is encouraged that you learn how to help classify her fertility signs or read the chart if possible. In the very least, you need to learn to respect your partner’s fertile window and not expect to ejaculate inside the vagina in the fertile window. I’m being blunt here. You will get used to “TMI” with charting! You can learn to understand the cycle by taking a class together. This is a great activity for bonding, and so that you have more equal responsibility in your family planning.
An easy way to get involved in your partner’s charting routine is to use a paper chart. I keep a paper chart on the bedside table. It is always visible. My chart is pretty easy for my partner to read because the “baby” symbols mean possible fertility. You could do this with any method. Sit down together when you record the observations. Have your partner to explain what the fertility status of the day means.
This is an example of a paper chart on heavier cardstock. The days with babies are possibly fertile. Other days are available to use when the rules allow it. Charting on paper is a great way to share your chart with ease.
But Why Would I Attend a Class or Learn About Charting if I’m NOT the Female Partner?
Because you want to be a good, supportive partner!
When you understand your partner’s chart, you understand the chance of pregnancy that you both have. This can prevent mistakes from occurring if there is more than one set of eyes on the chart. When you become attuned to your partner’s menstrual cycle, you will also begin to realize why their mood might change throughout the cycle. This is fantastic for relationship communication. Your partner is not perfect. They may make mistakes when charting. Two is better than one for catching these!!
How Will We Avoid Pregnancy in the Fertile Window?
One of the first things you will learn when reading a fertility awareness book or taking a class is that you are expected to abstain from penis-in-vagina sex in the fertile window.
The reason for this is simple: it is only possible to get pregnant in the fertile window.
If you have penis-in-vagina sex in the fertile window, there will always be a chance of pregnancy. If you are avoiding pregnancy, this means that sex in the fertile window could result in an unintended pregnancy.
During this time, it is suggested that the couple work on other aspects of the relationship. Go on dates, cuddle, talk, play games.
If you decide to break the rules by having sex, you should be prepared for the possibility of pregnancy.
For Catholics, this is the only “licit” option for the fertile window.
For non-Catholics, oral sex and sex involving hands is safe in the fertile window as long as no semen ever gets near the vulva or the vagina. If semen touches this area, pregnancy can occur.
To determine how you will proceed in the fertile window, you and your partner should place yourself on the intentions scale. In the context of fertility awareness, intentions means how open you are to pregnancy.
The basic possible intentions follow. Select which is most appropriate to you as a couple. TTA means “Trying to Avoid” a Pregnancy.
TTA Seriously Avoiding: For these people, an unintended pregnancy may be devastating, whether to health, the relationship, or finances. A pregnancy is being avoided very strictly. These people should adhere to the rules of their method as closely as possible.
TTA Regular Avoiding: For these people, pregnancy is being avoided and the rules are followed. A pregnancy wouldn’t be convenient, but it would not endanger their life.
TTA Loosely Avoiding: For these people, a broken rule isn’t the end of the world. They may do strategic risk-taking like breaking rules on the cusp of the fertile window, or using something like the withdrawal method in the fertile window. They are not actively seeking a pregnancy, but they are okay with some chance of it happening.
TTW Whatever Happens: For these people, pregnancy would be okay whenever it happens. They break whatever rules they want. They aren’t actively timing sex for the most fertile days, but it might happen.
TTCTrying to Conceive: For these people, the rules do not have to be followed. They actively try to have sex in the fertile window.
You and your partner should discuss this scale and decide where you land before utilizing the fertility awareness method for sex.
What If We Decide to Use Barriers in the Fertile Window?
Remember, while you are fertile 24/7, your female partner is not. It is really important that if you are avoiding pregnancy that you respect your partner’s fertile window.
Some couples decide to use condoms, the withdrawal method, or diaphragms in the fertile window.
The most likely time for a barrier to fail is in your fertile window. After all, you aren’t using them at the other times of the cycle.
I personally believe that a couple has the right to make an informed choice in the fertile window. In particular, the male partner should realize that he is the one putting on the condom or pulling out. If he fails to do either correctly, a pregnancy can result. If you use these methods, do the research and inform yourself about how to use them correctly and what their efficacy is. If you are okay with this risk, you can use barrier methods. At the point you use a barrier method – you are outside of correct use for the fertility awareness method. Always remember that. An unintended pregnancy would be classified as a user error or barrier method failure.
How Long Does it Take to Practice Fertility Awareness Confidently?
On average, you will want to do at least 3 to 6 cycles of follow-up with an instructor to be completely autonomous and confident in charting. When you work with an instructor, you may be able to start utilizing the method to avoid pregnancy as sooln as the first cycle charting! (This is assuming that your partner has been diligent in their charting).
If you have PCOS, are coming off hormonal birth control, or are breastfeeding, you may need close instruction for longer. The Billings Ovulation Method recommends following up until the third ovulatory cycle postpartum. This could take a year or more if fully breastfeeding.
To Male Partners:What Advice Would You Give Male Partners Who Are New To Fertility Awareness?
These responses are taken from a 2019 survey I did on the male partners of FAM users. Enjoy!
“At first it seems backwards since science has a simple fix for conception: hormonal birth control. Some women are fine on hormonal birth control. Some can be really crazy on it. With some women, it can even kill their sex drive. With mine, she becomes so crazy that it kills both of our sex drives. So we’re doing this weird fertility awareness thing. Here’s my advice if you have a woman like mine. Even though she’s so beautiful and sexy that you just want to risk ejaculating in her to possibly get her off, you can’t do it with this. Yes, it puts more pressure on you to wear a condom and/or pull out, but at least your wife isn’t batshit crazy. And she’s still horny. So it’s worth it. Plus you learn a lot about the female body because I guarantee she’ll keep you up at night telling you about it lol. So don’t complain. We’re still getting laid. Unlike our friends who’s wives are on the pill or IUD. It just puts more pressure on us to prevent a baby. If she gets pregnant again, it’s probably our fault with this. And I’m ok with that. War Eagle!”
“You will wish you had always known this information. Test your pre-cum under a microscope for sperm if you are going to use withdrawal.”
“Knowledge is power and pleasure.”
“To do the research to fully understand the anatomy and physiology which will give you confidence in trusting the fertility awareness method.”
“Good luck m’a friend.”
“Embrace it.”
“Don’t be afraid to ask questions!”
“Be patient and understanding whilst always at least attempting to understand the technicalities surrounding the practice of the method.”
“Listen.”
“Read as much information as you can and stay informed.”
“Trust your partner, but do some cursory research as well. You both need to understand it to trust it.”
“Learn the actual science (as in the research literature) behind these technologies. Much of the medical establishment unfortunately has both insufficient and badly-outdated knowledge about FAM. Also, such will only be successful if the couple are both wholly on-board and possess the necessary knowledge, discipline, and self-control to utilize the method(s) correctly, whether trying to conceive or to avoid.”
“Get ya woman on it like yesterday.”
“Talk to your significant other and learn from her.”
“Learn about which days are the best to get pregnant; if you want to get pregnant together there is a way to learn the best days with a good degree of certainty. I think other men could benefit from learning this information about their partner.”
“Learn how the world works, and use that knowledge.”
“Listen to your woman and trust what she says about her observations. It’s not like the guy is the one using the method, but it’s good to be aware of it.”
“If you think it’s burdensome, remember the health and relationship benefits far outweigh the daily minor inconveniences. Encourage your SO to do the research to make sure they’re doing it right as well.”
“Shut up, pay attention.”
“If you are concerned about the well being of your partner, you’re more likely to succeed in supporting her and have an involved role in fulfilling both your reproductive goals through fertility awareness.”
“Be patient.”
“Take a lesson yourself or attend one with your partner, you are only going to trust it if you understand how it works yourself. When you actually see that it makes sense, it’s not some weird alternative thing, you can trust it a lot more.”
This resource is a simple overview of the rules with examples. It links to other resources on understanding the female and male reproductive system. This is a good, fairly quick read for men who want to understand the basic rules.
Jessie discusses her symptoms that lead her to stop taking hormonal birth control. She then does a brief overview of how the fertility signs change throughout the cycle and how sperm life plays into fertility.
This also leans religious but may be useful for men who are having trouble adjusting to avoiding unprotected sex in the fertile window.
“Use of Natural Family Planning (NFP) and Its Effect on Couple Relationships and Sexual Satisfaction: A Multi-Country Survey of NFP Users from US and Europe.” Front Public Health. 2017; 5: 42. Published online 2017 Mar 13. doi: 10.3389/fpubh.2017.00042
This is a recent scientific article that studied the effect of NFP on relationships.
Have you ever wondered what it was like to chart with the Marquette Method? This blog attempts to give an overview of what it is like to chart with the Marquette method (monitor/hormones only) for one cycle. Since I am in regular cycles, this is only an overview of what that looks like. Postpartum charting involves a whole lot more testing!
Day 1: Record Heavy Bleeding.
(This is an available day for safe sex based on my Marquette calculation rule. Marquette calculation rules rely on the earliest peak in the last 6 cycles minus 6. For me, this is Day 7, with Day 8 being automatically the first “unsafe” possibly fertile day. Any time of day is allowed within Marquette calculation rules).
Day 2: Record Heavy Bleeding.
Day 3: Record Heavy Bleeding.
Day 4: Record Medium Bleeding.
Day 5: Record Medium bleeding.
Day 6: Do absolutely nothing! My testing window opens on Day 8.
Day 7. Do absolutely nothing! My testing window opens on Day 8. This is my last day to have sex pre-ovulatory per the rules of the method.
Day 8: I wake up at 6:30am, pee in a cup, dip the stick for 15 seconds, and wait 5 minutes for the Clearblue Monitor to read my test. I get a “L” or low estrogen reading. The Clearblue monitor reads both estrogen and luteinizing hormones.
Day 9: I wake up at 6:30am, pee in a cup, dip the stick for 15 seconds, and wait 5 minutes for the Clearblue Monitor to read my test. I get a “L.”
Day 10: I wake up at 6:30am, pee in a cup, dip the stick for 15 seconds, and wait 5 minutes for the Clearblue Monitor to read my test. I get a “L”
Day 11: I wake up at 6:30am, pee in a cup, dip the stick for 15 seconds, and wait 5 minutes for the Clearblue Monitor to read my test. I get a “H” or high estrogen reading. This means that my real fertile window is likely opening and ovulation could be around the corner.
Day 12: I wake up at 6:30am, pee in a cup, dip the stick for 15 seconds, and wait 5 minutes for the Clearblue Monitor to read my test. I get a “H.”
Day 13: I wake up at 6:30am, pee in a cup, dip the stick for 15 seconds, and wait 5 minutes for the Clearblue Monitor to read my test. I get a “H.” Based on having high quality mucus (which is not required to notice for monitor only), I crosscheck with a LH test because I know ovulation is likely approaching soon.
Day 14: I wake up at 6:30am, pee in a cup, dip the stick for 15 seconds, and wait 5 minutes for the Clearblue Monitor to read my test. I get a “P.” This means the monitor has now detected my LH surge. I crosscheck this same urine with another LH cheapie test, and it is also positive.
This means I have peaked for the cycle! All other readings after the “P” are automatic, and I do not have to take any other tests. Marquette requires me to meet PPHLL before resuming intercourse on the day after the second L.
At this point, if I desired, I could be done charting for the whole cycle! This means that I only had to really chart for approximately 7 days this cycle. How easy is that?!
If I desire, I could also take a Proov progesterone test around the second L at the end of my count. This would provide proof that the hormone progesterone has taken over.
Close up of a Body Literacy Collective “Read Your Body” chart with Marquette markings.
Some of the downsides to this method could be:
The Monitor missing peak (happens in up to 10% of cycles and many people crosscheck with LH for this reason, or even add temperatures or Proov)
The Monitor will not tell you if you are going to ovulate early. The only way to detect earlier ovulation is to track cervical mucus very carefully.
The sticks are approximately $1.50 each. This could get very pricey for delayed ovulation!
The method may not be appropriate for people with very irregular cycles or elevated LH levels (some PCOS users may have elevated LH).
I personally crosscheck my monitor with Billings Method observations and Proov tests. You can read about charting with Billings here.
Disclaimer: Do not try to learn how to chart from this post. Everyone has their own unique cycle and this is just an example of charting with Marquette in a regular cycle. I recommend finding an official Marquette teacher here. Because the Marquette method uses the Clearblue monitor which is designed for trying to conceive, you will need to get instructions to use this monitor for avoiding pregnancy.
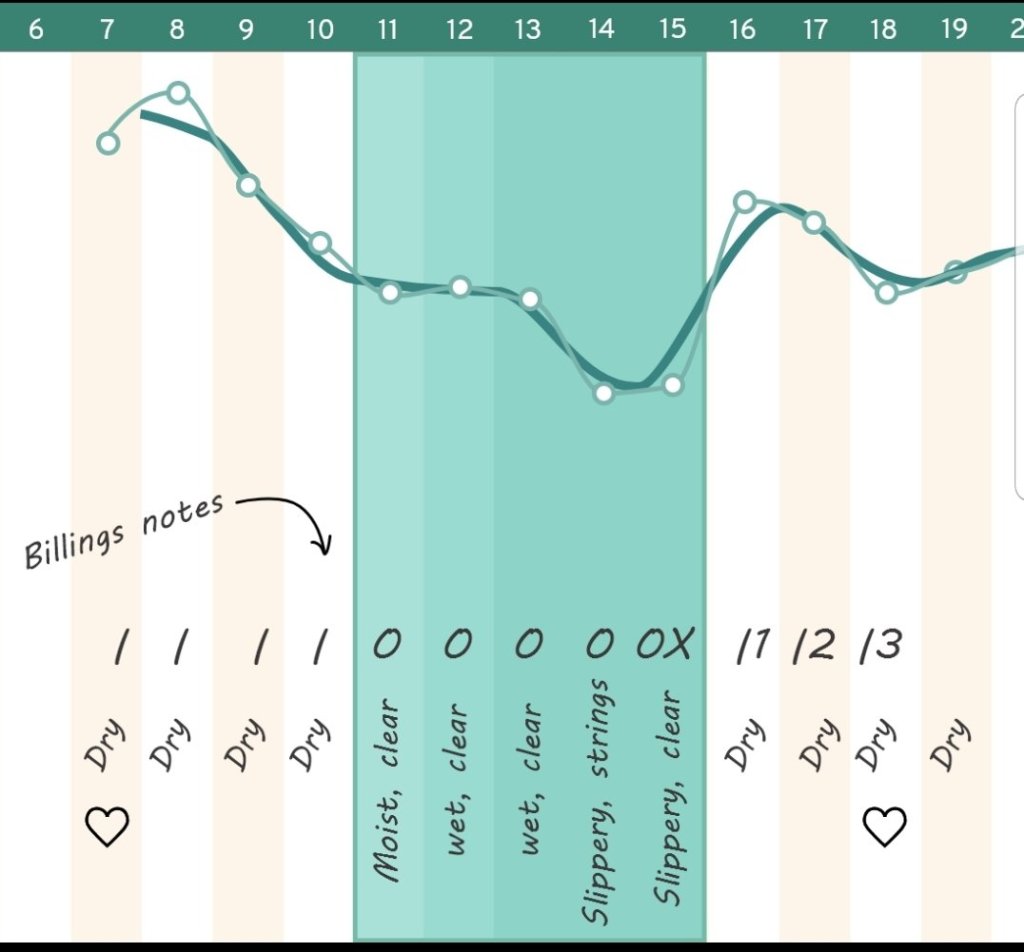
Have you ever wanted to know what it is like to chart with the Billings Ovulation Method? This blog attempts to give an overview of what it is like for one individual to chart with the Billings Ovulation Method (BOM) over a single cycle. I go through each day of the cycle and explain my overall charting habits. All times are just approximate. I get personal and discuss some challenges I experience with natural family planning. BOM involves tracking sensation felt at the vulva along with the visible appearance of cervical mucus as a person goes about their day to day activities.
Day 1: Record heavy bleeding. Heavy bleeding feels wet. Done! Users are not allowed to use heavier days in the Billings method when avoiding pregnancy. This is a true day one of a cycle because it was preceded by a Billings peak day.
Day 2: Record heavy bleeding. Heavy bleeding feels wet. Done!
Day 3. Record medium bleeding. Medium bleeding feels wet. Done!
Day 4: Very light bleeding. It is now possible to observe my basic infertile pattern of dry.
8am: I feel dry and see a small amount of blood.
10am: I still feel dry.
8pm: I still feel dry. I see no mucus. Sex is allowed in the evening of this day. We use this day.
Day 5: Extremely light bleeding. Technically this day is not allowed for intercourse since I used the day before and Billings method rotates alternative evenings. We use this day anyway #rulebreaker
Day 6: I feel dry. I do not see anything. I record this day as “possibly fertile” since I broke a rule and used the day before. Every day after intercourse gets this white stamp in the pre-ovulatory time of the cycle.
Day 7: My basic infertile pattern of dry is still there! I notice nothing the entire day in the bathroom and my vulva sensation is dry. Sex is allowed in the evening. I consider my evening 8pm because I go to bed around 9pm on average. We use this day.
Day 8: I feel dry all day and see nothing. However, this day is not allowed since Billings alternates days. We skip this day.
Day 9: I feel dry all day and see nothing. However, we do not use this available day because we are both tired. It happens!
Day 10:
9am: I feel a bit moist. I don’t see anything when wiping in the bathroom.
11am: Still feel moist. I do not see anything in the bathroom.
2pm: Still feel moist. I do not see anything.
4pm: Still moist. Nothing seen.
4:45pm: Walking to my car from work. Still moist!
8pm: Overall observation for the day is moist. I record it. The fertile window has opened. This is known as the point of change.
Day 11:
7am: I feel moist as soon as I walk to the bathroom. I see very scant clear mucus on the tissue.
I do not see or feel anything for the rest of the day.
8pm: Overall observation for the day is “moist, clear”
Day 12:
7am: I feel moist, but see nothing.
10am: I feel moist, but see something white.
8pm: The feeling remains the rest of the day. I record “moist, white” for the day.
Day 13:
7am: I feel dry.
11am: I still feel dry.
1pm: I feel wet sensation when walking to my office. This is a change, so I keep that in mind.
I feel damp the rest of the day. I never see anything in the bathroom. I record “wet” as the most fertile sensation that day.
Day 14:
6:30am: I immediately feel moist.
9am: I see long clear strings when wiping in the bathroom.
11am: I have a wet sensation when walking around.
3pm: I walk around my work place. I still feel moist.
5pm: I see clear strings again.
8pm: I record “wet, clear strings” on my chart.
Day 15:
7am: I feel a gush as soon as I wake up. I do not see anything in the bathroom.
9am: I see scant, clear mucus on the tissue when wiping.
11am: I feel very wet walking around my work place.
1pm: I do not see anything on the tissue.
3pm: I do not see anything on the tissue.
5pm: I feel wet sensation while making dinner.
8pm: I record “wet, clear” as my observation for the day.
Day 16:
7am: I do not feel or see anything when waking up.
9am: I still do not feel or see anything.
12pm: I go for a 20 minute walk. When I get back, I feel slippery sensation. I go to the bathroom and see copious amounts of long, clear mucus.
8pm: I felt slippery the rest of the day. I record “slippery, long clear” on the chart.
Day 17:
6am: I feel dry when waking up.
8am: I don’t see anything or feel anything.
11am: I don’t see anything or feel anything.
8pm: The day was nothing felt, nothing seen all day. I record dry. This means yesterday was my peak day because it was a changing and developing pattern ending in slippery followed by an abrupt dry up to no longer wet or slippery.
Day 18 and Day 19:
I have the same experience as day 17. I pay attention all day and observe no mucus or sensation.
Day 20:
Ovulation is expected to be over and the cervical mucus plug has re-closed for the cycle. Sex is available any time for the rest of the cycle until day one of menstruation occurs. I can chart, but it is not necessary to wait until the evening and observations are less important as sex may interfere at any time.
Day 28: I record heavy bleeding and the rules restart.
Real Talk: Diffulties / Obstacles With Billings Not Seen on the Chart
These are things that I find can be difficul in my own personal experience. I know that people in really long cycles or with other irregularities may have different issues than me.
Challenge One: Alternative evenings only can be a struggle, and it seems even harder for me right before the fertile window opens due to my mood at this time of the cycle. This follicular phase is much longer for me than my luteal phase on average, and this means alternative evenings is the rule for most of my cycle. If someone has a partner with a conflicting schedule, this can especially be offputting. I think anyone who is going to practice this method should consider whether this is practical for their lifestyle.
Challenge Two: Expected abstinence in Billings can be hard, and I have fairly short fertile windows on average. I originally practiced sympto-thermal, and I switched to Billings when I realized that overall consecutive abstinence was much less overall (for my own cycle, Billings: 9 days, Sympto-Thermal: 14+ days). I tend to break some rules still, but this is much more suitable for my fertility intentions level than sympto-thermal.
Look out for my next blog on “A Day in the Life of a Marquette User.”
Disclaimer: Do not try to learn how to chart from this post. Everyone has their own unique cycle and this is just an example of charting with Billings in a regular cycle. Please reach out to me if you would like to learn this method with me as your guide. Alternatively, you can find a teacher here.
The kegg device draws a fertile window to give you the best days for conceiving a pregnancy based on the electrolyte levels present in the vagina. To use this device, someone would insert kegg into the vagina in the same two hour period of time during the day. kegg takes approximately two minutes to give the user a reading on the graph. As a bonus, it also gives you the opportunity to do kegel exercises while using it. Click here to read an article on the science behind kegg.
This product is an exciting development in the femtech field because it actually does read a real-time fertility sign. Cervical mucus is completely necessary for natural conception to occur. Without the presence of cervical mucus in the cervical crypts, sperm cannot to get to their destination to reach the egg. For this reason, anyone trying to conceive needs to track cervical mucus or use an alternative device such as Kegg (or a device that reads estrogen levels) in order to time intercourse for when they are most likely to conceive.
Here’s what Kegg looks like!My kegg values compared to my Billings Ovulation Method cervical mucus observations. I believe that the kegg was highly correlated with my actual fertile window based on a traditional fertility awareness based method!
Who is Kegg right for?
It is important to know that kegg is not suitable for avoiding pregnancy. It is designed to find the most suitable days for conception. For those avoiding pregnancy, the fertile window has to be much longer than the window what the kegg gives. Until kegg has been studied for pregnancy avoidance, I cannot recommend it as an alternative to cervical mucus checks which must be made multiple times of day until the evening when someone is strictly avoiding pregnancy.
kegg may be right for someone who wants to conceive without needing to take a class or read a book on cervical mucus. In my experience, for the most part, it detected my most fertile days in a way that would likely lead to conception if used.
kegg may not be right for you if you have a very erratic schedule. Because it has to be used in the same two hours and cannot be used up to 8 hours after sex, this may make Kegg harder to use.
Calendar methods get a really bad rap in the fertility awareness communities. A lot of this is for a very good reason. When the calendar rhythm method was discovered in the 1930s, it was revolutionary. However, since then, we have discovered real-time fertility signs such as cervical mucus, basal body temperature, and urinary testing.
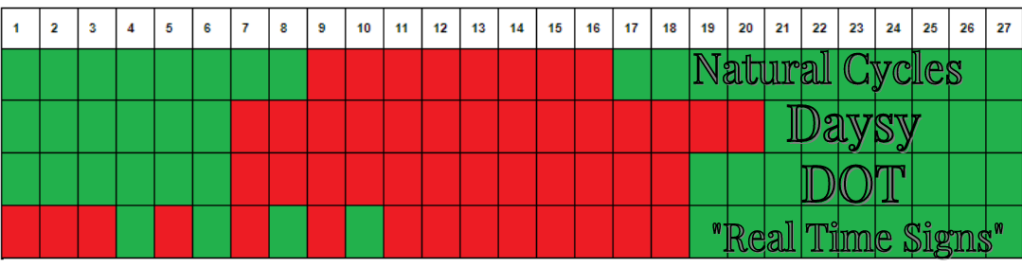
To illustrate why calendar-based rules can be both risky and occasionally line up with real-time signs, I charted with three calendar-based methods for opening the fertile window versus a method with real-time fertility signs only (specifically I used the Billings Ovulation method for my real-time method).
In the first line, you will see the Natural Cycles method. This method relies on basal body temperature as its only required real-time sign. Unfortunately, basal body temperature can only tell you when your fertile window closes, not when it opens. Temperature has no predictive qualities for letting you know if you are going to ovulate at a different time than normal.**
With only 3 cycles of my previous data, Natural Cycles gave me until day 8 as safe for this cycle. What Natural Cycles doesn’t know is that my cycles range from 24 to 30 days long over a calendar year. For this reason, it can be quite risky some cycles for me to be allowed safe sex until day 8. The fact that this cycle happened to line up is merely a coincidence! This coincidence can cause a confirmation bias when people use this app and do not get pregnant. If you are seriously avoiding, be wary of any method that doesn’t allow you to crosscheck the opening of your fertile window.
Natural Cycle also closed my fertile window in an incredibly risky manner. It told me I was safe on the morning after my real-time sign of “peak” day. In fertility awareness based methods, “peak” is the highest level of fertility you can get in a cycle. The two days following Peak day also have a significant chance of ovulation occurring. Every time I have used Natural Cycles (here is my previous try with it last year), it gives me a very risky closing to the fertile window.
Here is my full chart from Natural Cycles this time:
Natural Cycles app
Next up on the chart above illustrating my safe days is the Daysy thermometer. Daysy is a thermometer that relies on calendar based rules and potentially earliest temperature shift based rules to open the fertile window. In my two experiences with Daysy, it has been much more conservative than Natural Cycles. Daysy does learn over time, so it is possible I could have a risky day with it in the future, but so far I have not had any risky days with Daysy.
You can see in the image above that Daysy confirmed ovulation last out of all of the methods. I believe this is because my temperature shift was a bit erratic and because the device does not allow the user to mark temperatures questionable (I had two that were marked questionable for my own manual interpretation).
Daysy does not rely on anything except cycle length and temperature shift timing to open the fertile window. For this reason, Daysy can be risky if you ever have a very early ovulation. It can also be risky if the user is not careful about only taking their temperature when it is not disturbed, or if the device misreads a temperature shift. In my experience, Daysy tends to be much more cautious than Natural Cycles.
Daysy Chart
My third line is a true calendar only method. DOT has over a year of my data; however, the prediction has only given me one extra safe day during my whole use of the app. DOT is entirely based on the calendar method. However, interestingly DOT got higher efficacy than Natural Cycles in their study. Here is my DOT chart below
While I do not recommend the calendar method to most charters, this app can be useful for period prediction or for birth control if you are okay with an unintended pregnancy if you were to suddenly have a longer or shorter cycle. Users for DOT must have no more than 8 days variation in their cycle per calendar year.
In the example above, DOT actually gave me no risky days whatsoever. Again, this is a coincidence that it seemingly lined up with other signs. At any time, cycles can always change.
DOT the app
Finally, my main method is the Billings Ovulation Method. Billings relies only on real-time fertility signs. This means that they reject any calendar-based thinking, including the idea that menstruation is automatically safe. My Billings chart was based on when cervical mucus opened the fertile window (cervical mucus is what helps sperm survive) and when cervical mucus peak rules closed the window (when sperm can no longer access the cervix because ovulation is over and the cervical mucus plug has closed).
I always recommend real-time fertility signs to anyone who wants very high efficacy, the least amount of consecutive abstinence, who may be in regular or irregular cycles, and who want to understand their body and their health on a more deeper level. Here is an example of a Billings method chart. The babies represent possibly fertile days.
Conclusion:
I hope this post helps you think critically about whether calendar-based methods for opening the fertile window are right for you!
Here is a breakdown of efficacy for these methods:
**Some modern fertility awareness methods use the Doering Rule to set the opening of the fertile window. This can be very safe and yield high efficacy. Doering is based on the earliest temperature shift of all time (not just the last year).






































You must be logged in to post a comment.