It’s somewhat embarrassing to admit, but I find it hard to bring fertility awareness up to people in real life who haven’t heard of it before. For me, the awkwardness is their reaction to the name and what they think it entails.
Something about “fertility awareness” evokes something for some folks that is akin to “hippy” or “new age” type of connotations.
On the other end, some folks will think that this term means the calendar method or the rhythm method. This is partially because most people don’t know about the new science of real-time fertility signs. The other reason people think this is because most people who claim to be practicing a fertility awareness method are still doing some kind of bleeding tracking focused method. It’s truly a small percentage of us who are using a evidence-based real-time fertility sign method like Sympto-Hormonal, Sympto-Thermal, or Cervical Mucus only methods.
“Fertility” evokes conception for many folks. It also isn’t the correct word. We can only know if we were truly capable of fertility that cycle retrospectively when a pregnancy occurs, or if the cycle was visibly fertile by counting the luteal phase. I’ve seen a researcher say the correct term might be “fecundity.”
“Awareness” makes me think of some type of campaign. And what does awareness mean?According to the OED, “knowledge or perception of a situation or fact.” This can sound like people are charting with their intuition, but we are not. Fertility awareness modern methods track tangible and measurable fertility signs (cervical mucus, basal body temperature, cervix) or hormone levels.
I also don’t want to tell people that I teach natural family planning. Something about “family planning” makes people assume that the method is only for those who want to conceive, but a part of family planning is avoiding a pregnancy too. Then, there’s the religious connotation. I’m not Catholic, and I don’t just encourage abstinence because of religious compulsion.
Then, there’s the word natural. Natural is an incredibly subjective term. Some folks will see it and think this also means the withdrawal or pull out method. In the context of charting, it does not include withdrawal. According to the OED, one of natural’s meanings is “existing in or caused by nature; not made or caused by humankind.”
With this definition, do urinary hormones methods become “unnatural”? The hormones themselves occur in the human body, but you can only measure them with help from a machine. I’m not arguing against natural family planning including hormone monitors, but I do wonder if it makes sense to use that terminology.
My favorite terminology is “fertility awareness based methods.” Something about the word “based” makes it sound more scientific in my mind. I’ve seen some educators adopt this language to be more inclusive.
I’ve seen Samantha Zipporah talk about “conscious contraception” as a way to classify fertility awareness. I like the term conscious. Something about it sounds more sophisticated than awareness. I’ve seen it used in a few older academic articles. You can read them here and here.
I’ve also seen it called “Natural Fertility Control” or “NFC.” You can read an article with this terminology here. Some people will feel uncomfortable with the term “control.” In some ways, it isn’t control, because there is always a small chance of unintended pregnancy with correct use, and a larger chance of unintended pregnancy with incorrect use. I do think the self-knowledge gives the user a level of control over their choices more than other methods do. After all, with correct use, you will always know when you are possibly fertile, and then can make your decisions accordingly.
Many people think that having sex during menstruation cannot lead to pregnancy, but the answer is much more nuanced than that. It is possible to get pregnant during bleeding episodes, some of which may not be menstruation!
Was the bleeding truly menstruation?
Charting evidence-based fertility signs like cervical mucus, basal body temperature, and urinary tests are the best way to determine if you are ovulating. True menstruation should follow about 10-16 days post ovulation as indicated by a temperature shift or positive PdG test.
If you are not charting your cycle with a fertility awareness based method, your bleeding may not really be menstruation. Estrogen breakthrough bleeding may appear very similar to menstruation and is often indistinguishable without charting. This bleeding can be fertile, and pregnancy could result.
Day one of a true menstruation marks the beginning of the cycle.
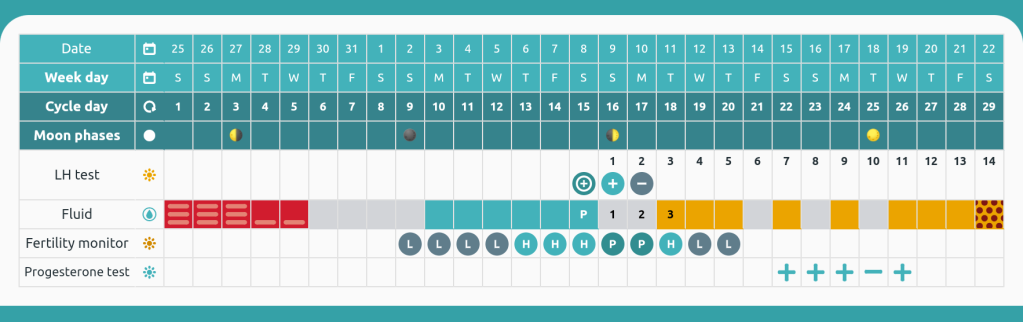
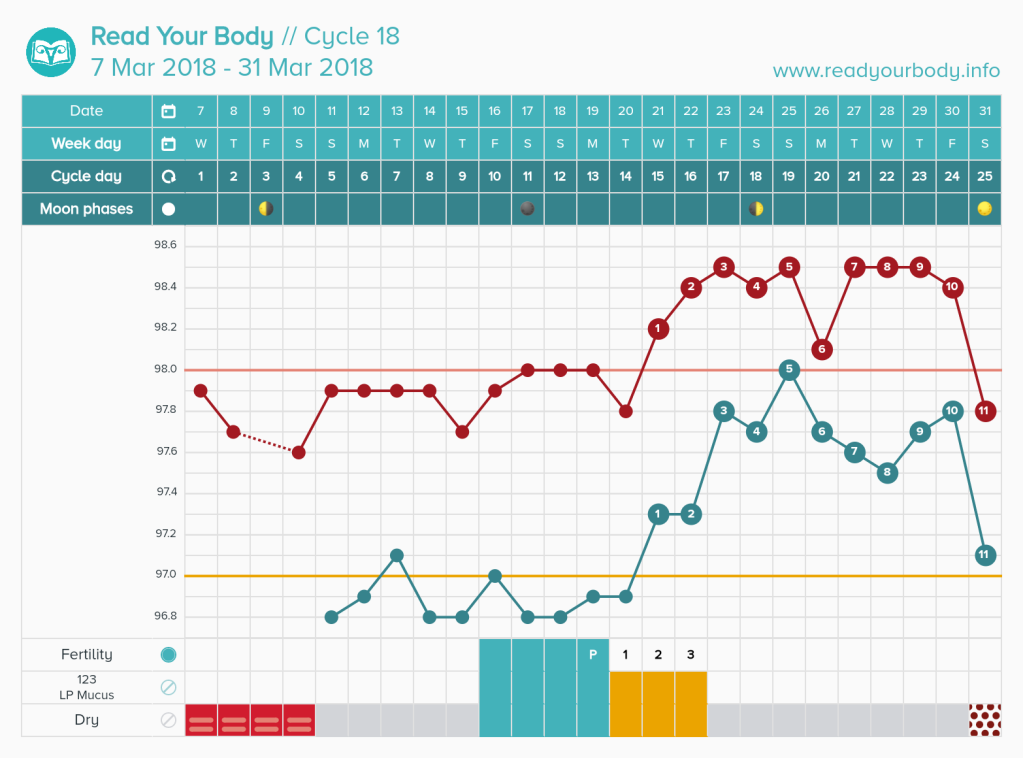
Day 1 is true menstruation because it followed a proven luteal phase. The current cycle confirms the next bleed will be menstruation because of the positive progesterone tests. This app is Read Your Body.
How long are your cycles? Better yet, approximately when do you usually ovulate?
If your cycles were 26 days or longer for the last year, it is unlikely you will become pregnant with sex during the first five days of the cycle.
Dr. Josef Roetzer monitored 5,807 cycles. He observed only one pregnancy before day 6 of the cycle. Her cycles were 22-27 days long.
Dr. Roetzer estimates that using the first five/six days is 99.8% effective for avoiding pregnancy. It is important to note that all of his cycles monitored had a temperature shift preceding menstruation. If you do not have proof that you ovulated before a bleed, it becomes more likely to conceive during bleeding.
Another way to determine the last infertile day at the beginning of the cycle is to use Dr. Doering’s rule. Dr. Doering subtracted 7 from the earliest first high temperature in the last year. For example, Sarah’s earliest first high temperature was day 13. Day 13 – 7 = Day 6 as the last infertile day of the cycle. This rule is always crosschecked with cervical mucus. Sperm may survive up to 5 days in cervical mucus, and any presence that has not been determined to be infertile through instruction should open the fertile window. The Doering rule is more personalized than automatically assuming the first five/six days are infertile.
In Dr. Frank-Hermann’s double-check sympto-thermal study from 2007, all three method failures were from day 5 intercourse. This study used the first five day rule and Doering rule. This study yielded an efficacy of 99.6%.
So am I safe to have sex during my period? Ask yourself these questions.
Did you confirm ovulation with basal body temperature, PdG strips, or a blood draw in the previous cycle?
Are your cycles longer than 26 days on average? Have you ever had a peak day before day 13 of the cycle?
If the answer to both of those is yes, you can probably have safe sex up to day 5 of your cycle.
If your answer is no, then you have a possibility of pregnancy.
What if I want to be more conservative?
Some methods like Billings, FEMM, and Creighton suggest not having sex during heavy days of bleeding when cervical mucus cannot be observed.
If you have a history of short cycles (less than 26 days) or want to add an extra layer of protection onto the beginning of the cycle, I recommend beginning observing vulva sensation and cervical mucus as soon as your bleeding has lightened enough to no longer need a tampon, cup, or regular pad. If you need only a panty liner or are only experiencing light spotting, you should beginning checking your cervical mucus and sensation throughout the day. At the end of your day, if you have observed no cervical mucus or sensation outside of your determined infertile pattern, this day is safe for sex. (DO NOT DO THIS WITHOUT LEARNING A METHOD. THIS BLOG IS NOT ENOUGH INFORMATION TO AVOID PREGNANCY WITH ALONE).
What if I bleed for more than 5 days?
If your menstruation lasts longer than five days, you should follow the instructions from the paragraph above. It is NOT safe to consider past day 5 automatically available if you are bleeding. You need proof by using cervical mucus or urinary estrogen tests that your fertile window has not yet opened past day 5 of the cycle.
What if I randomly have a short cycle?
Checking cervical mucus is your best back up. Cervical mucus should appear when the fertile window is opening for most charters. Many methods suggest no longer considering menstruation safe once you enter peri-menopause (can occur up to 10 years before menopause) because cycles may shorten at this time. If you notice that your cycles have grown shorter than 26 days, you may want to become more vigilant and stop automatically considering the first 5 days safe.
Conclusion
For the majority of people menstruating, using the first five days of a true menstrual cycle will not result in pregnancy. For a very small percentage, it may. I recommend charting with a real fertility awareness method (Sensiplan, SymptoPro, FEMM, Billings, Marquette, etc) to determine if your bleeding is actually menstruation!
Works Cited
Roetzer, Josef. “Further Evolution of the Sympto-Thermal Methods.” International Review of Natural Family Planning 1 (1977): 139-150.
Are you looking to simplify your basal body temperature charting routine? Is getting up in the morning just too hard to remember to take your temperature? Read on!
There are currently a few wearable basal body thermometers on the market such as iFertracker, Ava, and Tempdrop. In this blog, I will review the Tempdrop device. If you decide to purchase, use this link and get 10% off the device.
Unboxing Tempdrop!
Tempdrop is a wearable basal body temperature thermometer that came onto the market in 2017. Rather than setting an alarm, you can simply put this thermometer on before bed. You wear it around your upper arm (and it may be worn in a bra as well). It needs 3 hours of sleep to determine your basal body temperature. The device uses an algorithm to find your true temperature, regardless of how many times you have gotten up or whether you had restless sleep this night.
This device is very popular with shift workers, breastfeeding folks, and other people who don’t get a regular amount of sleep and wake up at different times, or just to those who don’t want to set an alarm!
Tempdrop holds 24 hours of data, and it must be synced at least every 24 hours or you will lose previous data. After wearing it for 15 days (as of March 2020), the algorithm will kick in. (If possible you should back up temp with oral basal body temperature for the first 60 days if you are avoiding pregnancy. If not, use a different method of protection). By day 60, the device will only change and make improvements to the last 2 temperatures taken.
Once you wear it, you will need to sync it to an app to see your temperature. Tempdrop has its own app, but I highly recommend using Read Your Body (pictured below) instead! This app is customizable for every method and can be synced to Tempdrop.
My Experience with Tempdrop
Tempdrop is red and oral temperatures are blue! One perk of oral temperatures is that sometimes I can skip taking my temperature, while with Tempdrop you do wear it daily for best results.
I used the Tempdrop device for almost 12 months. I found my oral temps to be more predictable and more steady when observing my own trends over time. I get very steady or repeating temperatures with oral charts most of the time.
However, I am not a shift worker, so I will admit that I do not need Tempdrop like some people may do. I already have to wake up at the same time 5 days a week, and I don’t find it inconvenient to take my temperature on the weekend. My oral temperatures caught my shift earlier than Tempdrop did on two separate occasions. I have seen other people say that Tempdrop catches their shift sooner than oral temperatures, so this is really an individual thing.
If you are dedicated to using a sympto-thermal method and can’t get accurate temperatures otherwise, and you have tried trouble shooting your routine (vaginal temperatures, pre-warming the thermometer before taking it, using longest stretch of sleep), then Tempdrop may be your best option. You can use my code for 10% off, and I will get a small kickback. Thank you for using my code!
It can be hard to choose the right method for you. In this graphic, I have simplified the main signs, times of intimacy, and efficacies for the four methods that I am most familiar with.
As part of my charting journey, I have personally compared and charted with Billings, sympto-thermal, and Marquette. You can view my charting comparisons here.
The graphic is intentionally simplified. Method rules will vary, particularly if you are using a different protocol of the method or combination of signs. My Marquette example is for monitor-only rules.
Time of day for intimacy is very important to consider as a part of the decision making process. If you and your partner’s schedules don’t mix well, this may sway you towards another method!
Some couple like intimacy to feel spontaneous. If you never want to worry about time of day, Marquette is likely the best method to choose.
On the other hand, if you want your fertile window to be defined by cervical mucus, you may want to sacrifice any time of day sex for the flexibility of opening the fertile window that may come with using alternative evenings of the basic infertile pattern in Billings.
I recommend interviewing an educator and telling them your unique situation before committing to a method.
To find an instructor, I recommend using the Read Your Body Educator directory linked here. You can use it to find an instructor based on the fertility signs you want to chart, your location, price range, and more!
After menstruation, the majority of women will experience dry days. For these women, their basic infertile pattern is dry. Other women may experience a pattern of unchanging mucus, sensation, and discharge after menstruation. For women who experience this same UNCHANGING discharge, mucus, sensation pattern for three cycles in a row following menstruation, they may have a non-dry basic infertile pattern. The keyword here is unchanging; any changing pattern would not indicate a basic infertile pattern. This type of pattern should only be established under an instructor if someone is seriously avoiding pregnancy. For women who establish this pattern with a mucus-only instructor (either Billings or Creighton are options), this pattern has the same level of efficacy for avoiding pregnancy as a dry pattern. Some examples of this pattern may be continuous moist days, continuous sticky days, continuous white mucus, or others!
DO NOT try to use these days for unprotected sex without establishing it for a minimum of 3 cycles with an instructor (it may take longer than this). When using these days, intercourse should be rotated to every other day in the evening before bed.
What causes this pattern? In cycles less than 35 days, it is caused by bits of the G mucus plug breaking off. While the plug is breaking off, it causes the visible mucus or sensation. However, the rest of the plug is still blocked. This means this time of the cycle can be considered infertile if an instructor works with you to make sure it is the G mucus plug breaking off. In cycles longer than 35 days, it can be caused by a combination of the G mucus plug breaking off and estrogen’s effect on the vaginal walls causing a sloughing effect. Read more about the types of mucus here.
Sympto-thermal methods like Taking Charge of Your Fertility also mention a “sticky” dry basic infertile pattern. Methods like SymptoPro claim that women do take on an elevated pregnancy risk when using these days. As sympto-thermal methods are not as strenuous on mucus observations as mucus-only, consider this risk when deciding to utilize this pattern. Again, ideally if someone is avoiding pregnancy, they should reach out to an instructor before using these.
In either of these cases, experiencing any dry days following menstruation means that you do not qualify for a basic infertile pattern of non-dry in regular cycles. This pattern needs to be re-established with an instructor following hormonal birth control usage or pregnancy.
Irregular Cycles
For postpartum, perimenopausal, or people with cycles longer than 36 days, it is also possible to have a basic infertile pattern of non-dry after 14 days of the same UNCHANGING discharge, mucus, sensation. In addition, a combined basic infertile pattern is possible in the Billings Method. This should only be established with an instructor. For these transitions, the Billings Method is highly recommended.
In both regular and irregular cycles, working with an instructor can help you get more safe days for unprotected sex if you are experiencing a non-dry pattern.
I’m expanding my usual content to include book reviews of fertility, sexuality, birth control related materials. This is the first review in a series. The content will also be shared to my Instagram account.
Lactivism has been on my reading list for a while. As a fertility awareness educator, I run into a lot of breastfeeding glorification in online spaces. This book looks at breastfeeding from social and political perspectives. Jung outlines the ways that breastfeeding can be a privilege and how it should not be viewed as a moral imperative.
One of the most standout examples of breastfeeding related discrimination in the book is with WIC, a voucher system that lower income people who have a baby or are pregnant can use to purchase basics like milk, eggs, bread, and veggies. I was a cashier for close to 7 years, and WIC was always a really hard process due to the extreme restrictions on what can be covered by the vouchers. I often wondered the why behind WIC and who has access to what. Jung discusses how women who apply to WIC are pressured to breastfeeding exclusively if they want more food and benefits. What this pressure ignores is that mothers in the United States are not given maternity leave and may not be able to breastfeed exclusively for the suggested 6 to 12 months. In addition, all mothers may not be able to produce enough milk for their child or want to breastfeed exclusively if they have other duties (like providing for their family monetarily).
Jung also covers the pumping industry and workplace discrimination around pumping. I had no idea that the average pumping time to empty one breast is 30 minutes! She goes into detail about average pumping prices and time. This section is a must read if you are planning to pump at work.
On the flipside, Jung reviews the history of formula. This industry too is ridden with issues. One of the most shocking parts of the text discusses the promotion of breastfeeding over formula by organizations like La Leche League for mothers with HIV. Jung cites studies showing approximately 22% of babies in some cases have contracted HIV by 6 months of breastfeeding.
I highly recommend this book for anyone looking to learn about breastfeeding and formula from a more cultural angle. At 272 pages, it is a fairly quick read with all the eye-opening, suprising details about how organizations from WIC to La Leche League have promoted breastfeeding even when detrimental to mothers.
You may know that the Fitbit app has some built in menstrual cycle tracking features, but many people do not know that it has other features that may be useful for menstrual cycle tracking. In this article, I will review the pros and cons of the Fitbit app as it relates to cycle tracking for people who ovulate. For context, I use a Fitbit Charge III.
The most basic feature that Fitbit offers for cycle tracking is recording bleeding dates of menstruation and then displaying a predicted fertile window based on average cycle length.
The pink bar represents the length of menstruation. The blue bar represents a predicted fertile window. The flower symbol represents predicted ovulation.
The user needs to remember to input menstuation each cycle. Once it is inputted, Fitbit will generate the blue fertile window. This fertile window should NOT be used for avoiding pregnancy, as it is only based on cycle length and not real-time fertility signs like cervical mucus or basal body temperature.
Once menstruation is entered, it will also begin a countdown until your next predicted menstrual cycle.
Countdown until menstruation in the app.
Unfortunately, I do not find this basic feature very useful for anyone who has any cycle variation. Even though my cycle length has increased over the last year, Fitbit has not automatically updated my cycle lengths. The app does not appear to be very adaptive without user input.
In addition to tracking bleeding the app offers options for:
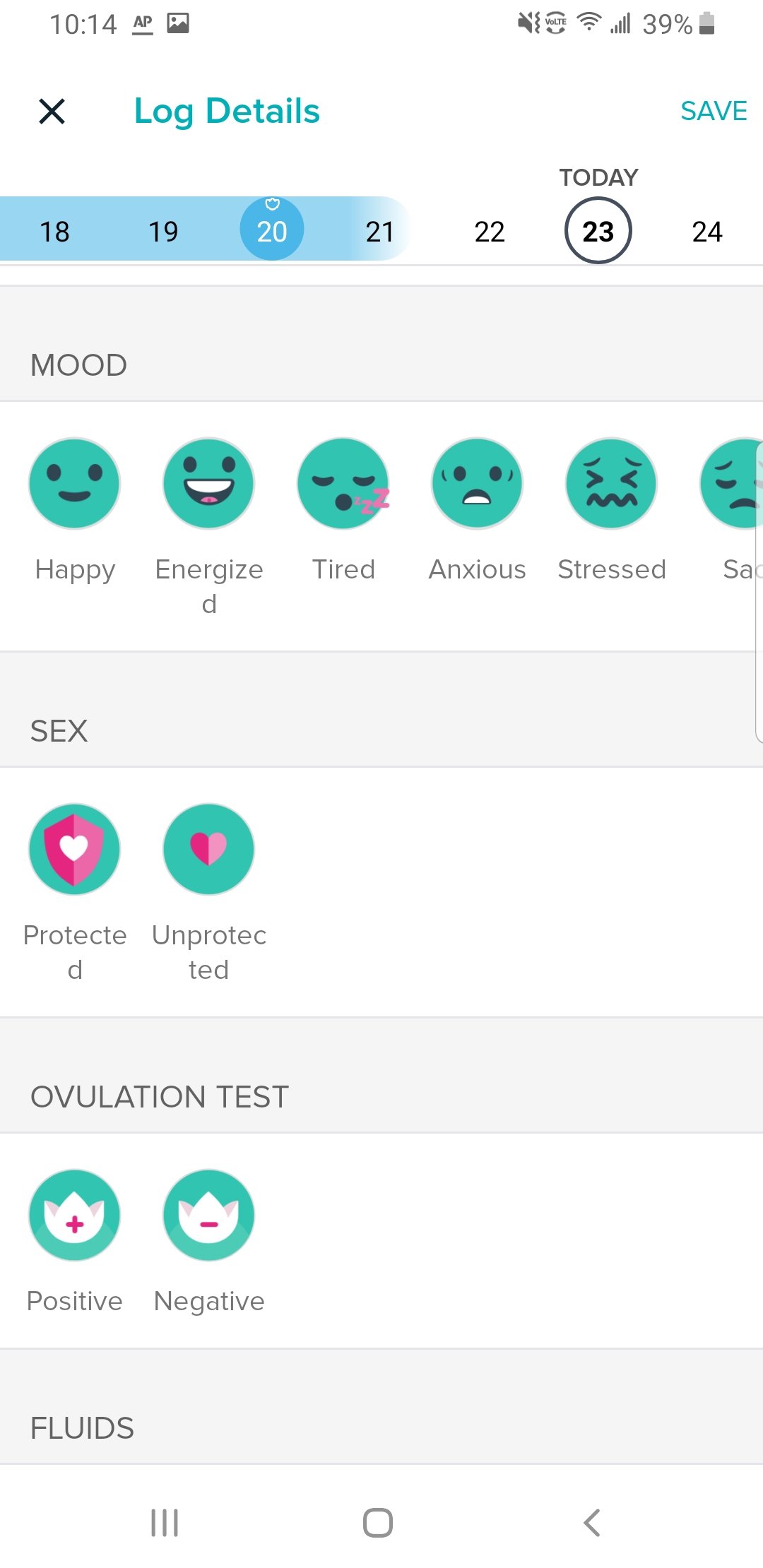
Mood
Plan B (morning after)
Ovulation tests (better called luteinizing hormone tests)
Cervical mucus (Taking Charge of Your Fertility categories)
Cyclical symptoms like acne
It is rather disappointing that the app does not include options to mark pregnancy when it occurs, especially since we know that this changes daily calories burned and heart rate, to name just two effected areas of the app.
Screenshots of other features.
A really cool feature that I do like is the ability to show cycle trends like flow intensity and cramps. The same screen that displays this will also let you scroll through all past cycle lengths.
In the settings of this screen, you can also decide to toggle off predictions. For people avoiding pregnancy, I do recommend either ignoring or toggling off predictions in the Fitbit app. The app allows you to choose your current birth control method as well.
Outside of the designed menstrual cycle tracking features, I want to highlight resting heart rate as a potential exciting thing to track for those who are not taking hormonal contraception. Why do you need to not be taking hormonal contraception to utilize the heart rate feature for menstrual cycle tracking? Hormonal contraception suppresses ovulation, and ovulation changes our heart rate charts!
You can see my heart rate falling during menstruation around April 10th, and then rise during my fertile window and luteal phase. Menstruation began when my heart rate dipped below 70 on this chart. Ovulation likely occured around the third raised heart rate in this close-up.
Heart rate in people who are ovulating is at its lowest point during menstruation, rises during the fertile window, and continues to be elevated in the luteal phase.
When heart rate begins to drop again, this is an excellent way to predict menstruation will soon occur. For example, I have been tracking my heart rate in Fitbit for 2 years, and I always bleed when my heart rate dips back down to 70 beats per minute after my luteal phase!
I do think this feature is worth tracking for anyone interested in a more precise period prediction than cycle length. If you have Fitbit premium, you can also find a setting for sleeping heart rate under restoration. This may be more steady than resting heart rate for some individuals.
The red line is sleeping heart rate converted to fit on a charting graph, and the blue line is resting heart rate. They rose near the time of possible ovulation as indicated by the positive LH tests on the chart.
Lastly, I want to address Fitbit temperature for menstrual cycle tracking. Unfortunately, wrist temperatures are not a compatible parameter for fertility awareness when it comes to avoiding or achieving pregnancy. It can be incredibly erratic. When we track temperature, we want the temperature as closest to the core as possible.
Fitbit does not give precise temperatures, instead it gives deviations from a range. I likely ovulated near 18, 19, or 20 on the photo above. While Fitbit did detect a slight shift, it is not particularly clear, and it dropped back down.
As depicted above, my luteal phase the previous month was extremely undefined, and I could not determine a confirmed temperature shift with it.
For now, I do not recommend Fitbit for precise temperature tracking. Instead, I recommend a basal body thermometer.
Conclusion
Fitbit offers some really unique options for cycle tracking, but it should not replace your birth control or fertility awareness method. The heart rate feature may be useful for identifying cycle phases, but the temperature readings are not suitable for tracking cycle phases.
Have you ever been curious what your fertile window would look like in multiple methods?
In this blog, I show 6 cycles with various fertility signs and method interpretation including: the sympto-thermal method (Sensiplan rules), Marquette method, the Billings Ovulation Method, and DOT (a calendar method that was recently purchased by Clue app and is a new FDA approved birth control). I chose to include representation for only studied methods of fertility awareness: sympto-thermal, sympto-hormonal, mucus-only, and calendar method.
All charts are from the Read Your Body app, a flexible app for all methods that I highly recommend!
Some things to know before reading:
Marquette allows sex any time of day within their rules. My calculation rule lasts until the end of day 7.
Sympto-thermal method allows sex any time of day during first 5 days of menstruation, but the first safe day in the luteal phase must be used in the evening. My calculation rule is day 5.
Billings Ovulation Method allows sex in the evenings only and on rotated days in the pre-ovulatory time of the cycle. Days of bleeding where mucus cannot be observed are not allowed. However, since you can have sex any time of day post-ovulation with Billings, sometimes cycle day 1 is available if you have sex before bleeding occurs.
DOT allows sex any time of day within their rules. It automatically opens my window on day 7.
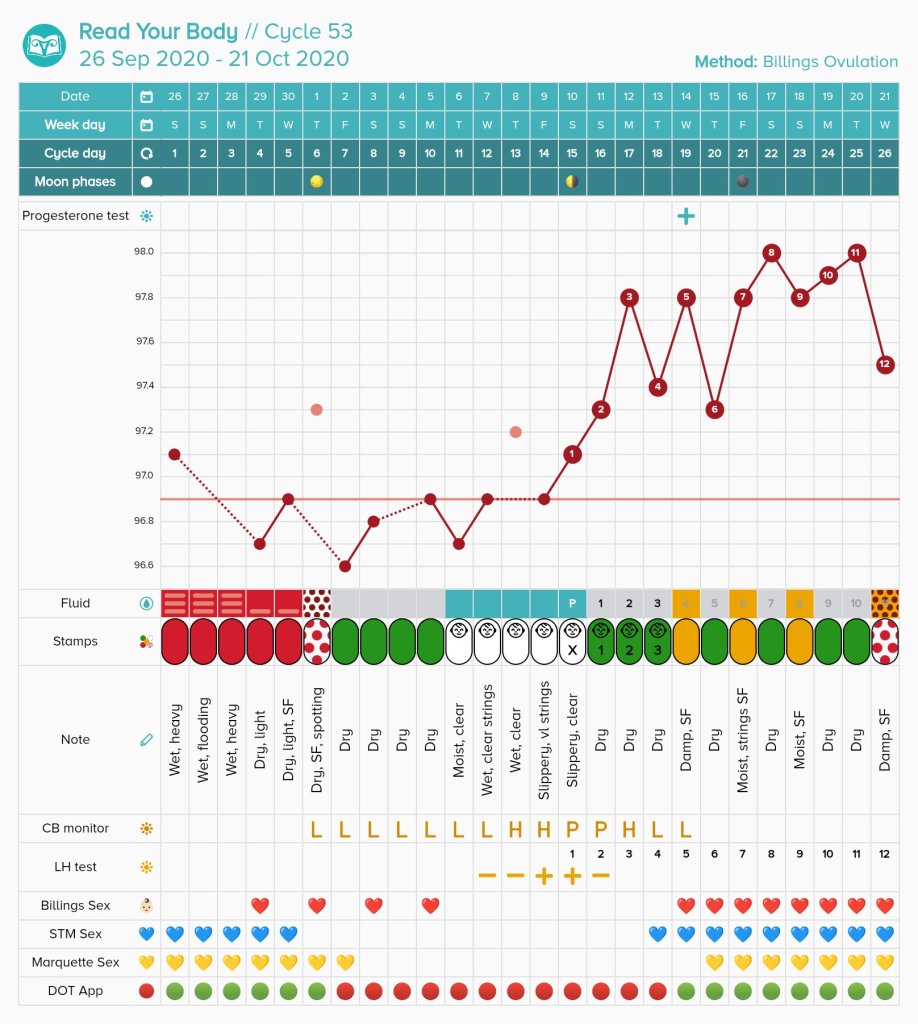
Cycle 53
Consecutive Fertile Window for Expected Abstinence:
Billings: 8 days
Sympto-thermal: 12 days
Marquette: 12 days
DOT: 12 days
General remarks: This is an extremely standard cycle in length and mucus patch (the average person will have a 5 to 6 day mucus patch when charting). I believe this is a great example of what methods would look like for someone of the average cycle length.
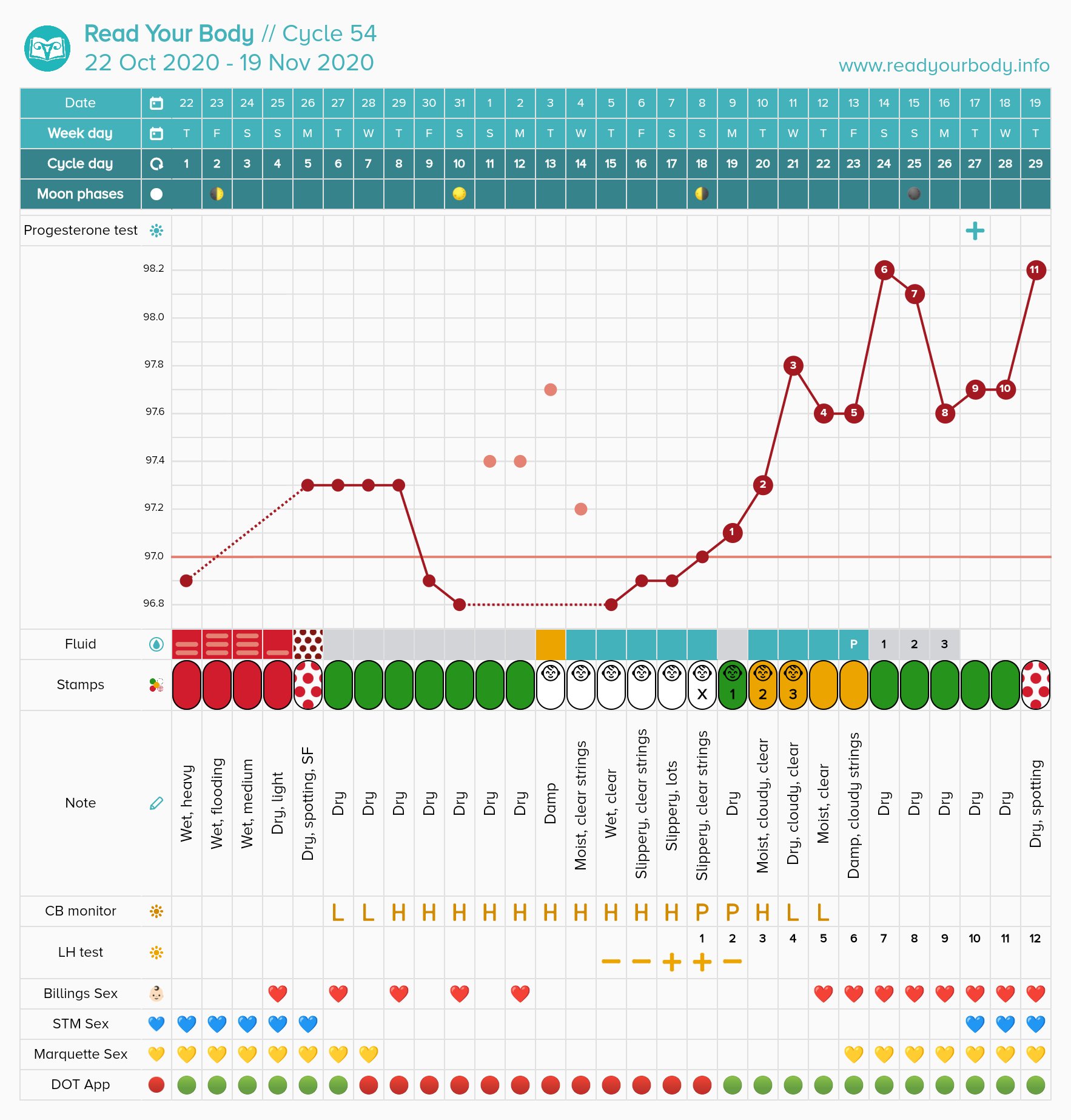
Cycle 54
Consecutive Fertile Window for Expected Abstinence:
Billings: 9 days
Sympto-thermal: 21 days
Marquette: 15 days
DOT: 12 days
General comments: My average coverline is 96.8 to 97.0, so regardless of earlier high temperatures and some illness I felt confident marking this coverline and temperature shift. Due to continous long, clear-ish mucus, my sympto-thermal peak was extremely delayed. Billings is a sensation focused method so I was able to mark my peak at an earlier time and have less expected abstinence.
DOT gave me a very risky day on this one. It is possible I could have been ovulating near the safe day. However, that would have only left 9 to 10 days for implantation and I had spotting, so whether this truly could have ended in pregnancy is up in the air. Even with well-timed sex, pregnancy will not always occur.
Cycle 55
Consecutive Fertile Window for Expected Abstinence:
Billings: 6 days
Sympto-thermal: 12 days
Marquette: 12 days
DOT: 12 days
General comments: This small fertile window in Billings might look scary to some, but it is not possible to get pregnant when the cervical mucus plug is truly closed. I have about one cycle like this every 13 cycles. I was also using the Kegg device during this cycle which is placed internally and reads electrolyte levels to determine the fertile window. It gave me the same 3 day dip for a fertile window, so I feel even more confident that those days were truly dry. I am missing temperatures on this one because my thermometer glitched and would not give me readings on these days. Sex day 1 was allowed because menstruation didn’t start until 5pm.
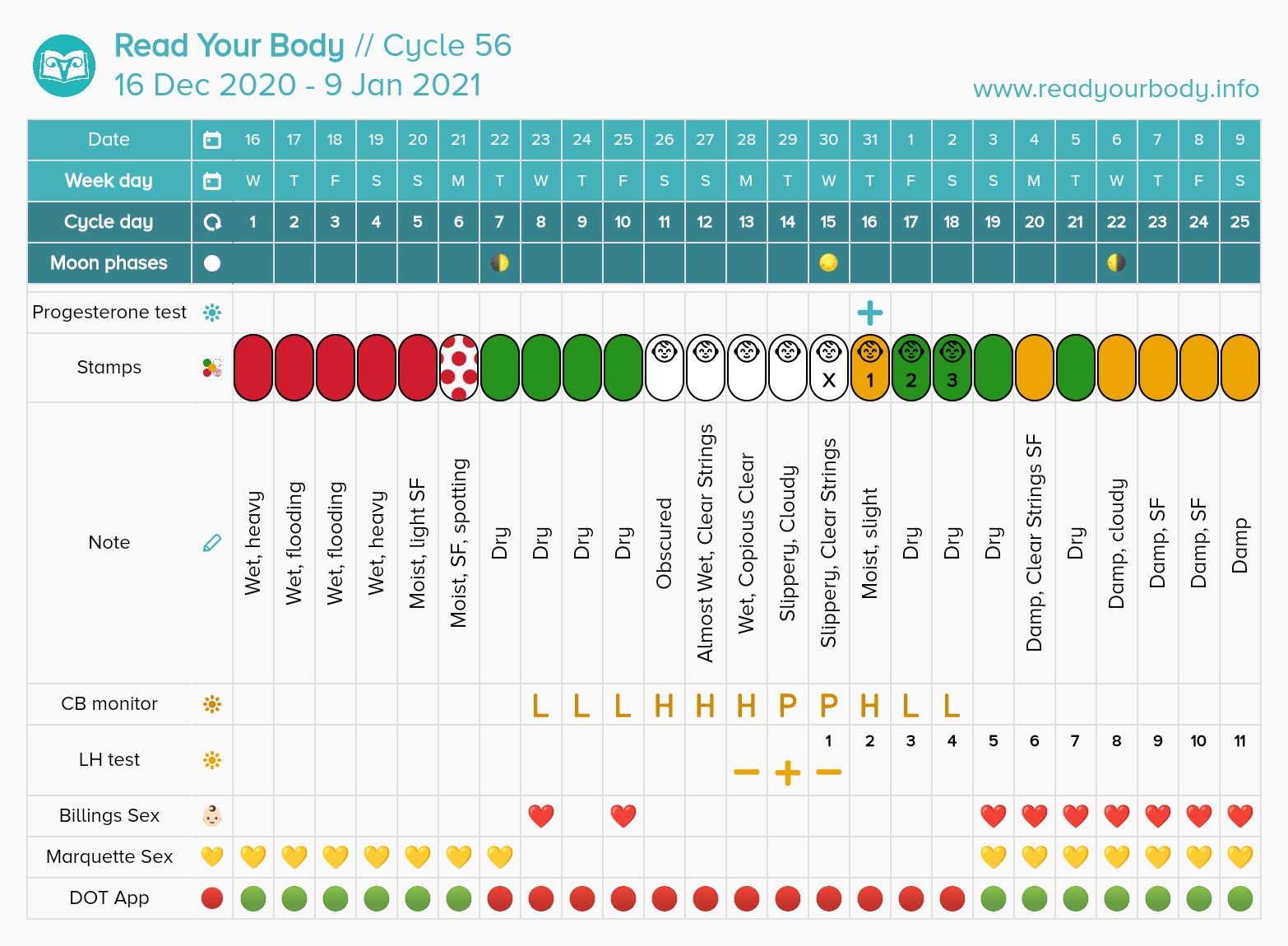
Cycle 56
Consecutive Fertile Window for Expected Abstinence:
Billings: 8 days
Marquette: 11 days
DOT: 12 days
General Comment: This was an extremely heavy period so I had no period days available in Billings. Even though the other methods gave me available days, I couldn’t have used them due to the pain, so ultimately the other methods didn’t really help out on more safe days.
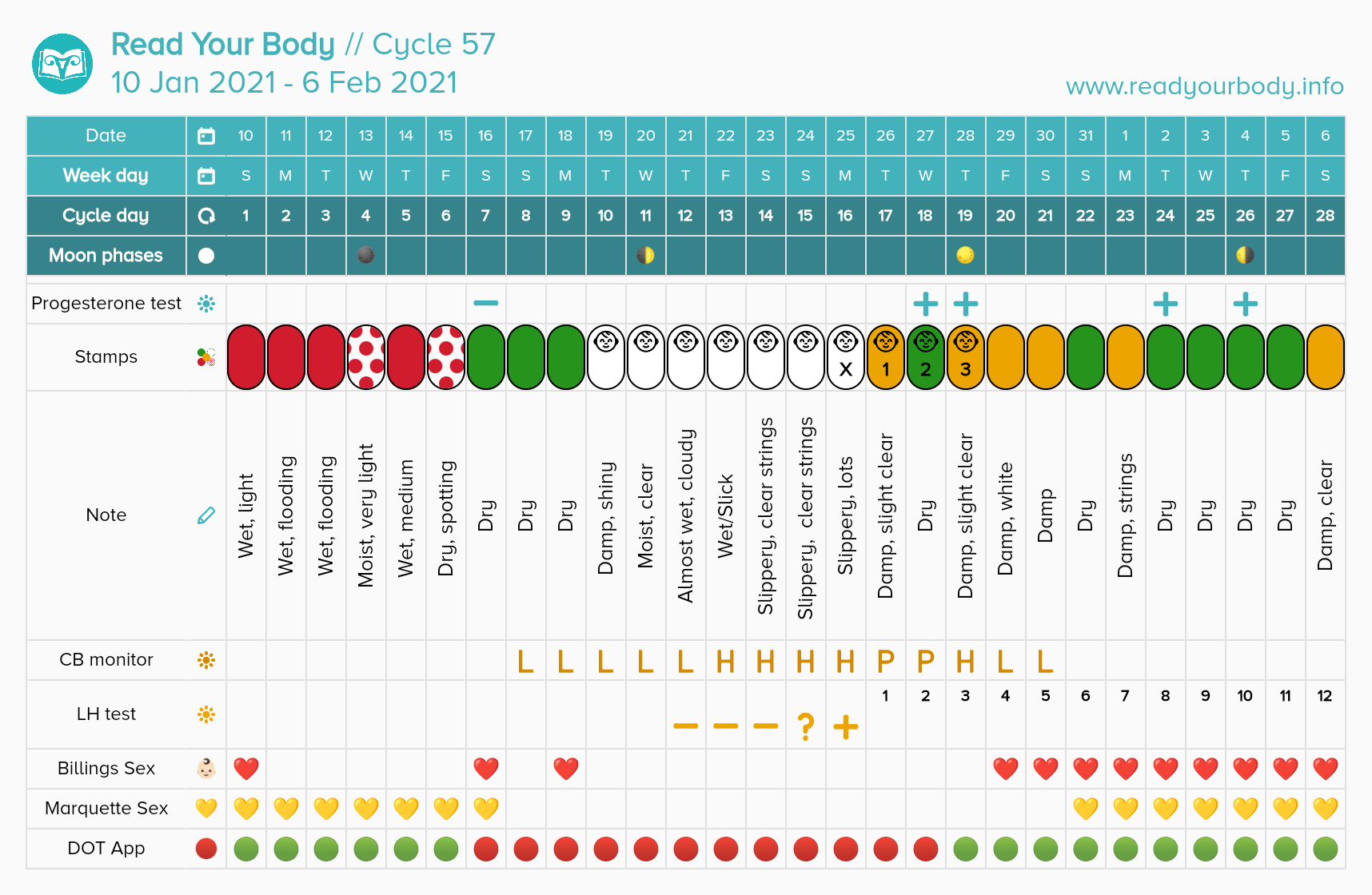
Cycle 57
Consecutive Fertile Window for Expected Abstinence:
Billings: 10 days
Marquette: 14 days
DOT: 12 days
Cycle 58
Consecutive Fertile Window for Expected Abstinence:
Billings: 9 days
Marquette: 11 days
DOT: 12 days
General Comments: Marquette monitor missed my peak on this cycle. It misses peak on up to 10% of cycles. I relied on meeting LH rules instead of the monitor. Sex day 1 was allowed because menstruation didnt start until 1pm.
Reflecting on What’s Best for Me
I’m currently on cycle 59 charting, and I have tried a ton of methods. Right now, my ideal method is Billings and LH tests as a bonus marker.
While it may appear that Billings gives less safe days in some instances, what is most important to me is having the smallest consecutive fertile window. Having less expected abstinence actually makes me more likely to follow the rules. I was completely unsatisfied with only being allowed period sex in the sympto-thermal method because I have period pain issues. That means that I basically had no safe days at all in reality before ovulation with sympto-thermal.
I originally felt very enthusiastic about Marquette method. However, after 6 cycles of using the Clearblue Fertility Monitor, I realized that it always caught my LH surge after the cheap LH tests. In addition, it missing my peak even once is frustrating for the cost of the product. For that reason, I have decided to stop using the monitor when I run out of tests. I can use a 15 cent LH test and get the period prediction aspect (LH is my most steady indicator).
The DOT app tends to give me a risky cycle whenever I ovulate late and have a shorter luteal phase. I do not rely on this for pregnancy prevention. Overall though, DOT has not given me many risky ways. I use it for long-term period prediction, and it is the most accurate period predictor I’ve ever used for planning months in advance.
What to Consider Before Switching Methods
1. Why are you unsatisfied with your current method? Is it the amount of safe days, or is it the routine that you don’t like?
2. Do you have medical needs that could be addressed by another method?
Sometimes the grass isn’t greener on the other side, but if you are like me and can’t have period sex or don’t want to have period sex, methods like Billings without calculation rules will almost always include more safe days if you are dedicated enough to learn the method and chart it accurately.
Folks in irregular cycles like in postpartum time or with PCOS may benefit from more flexible methods without calculation rules
*DISCLAIMER: DO NOT TRY TO LEARN FROM MY CHARTS. MY CHARTS ARE NOT YOUR CHARTS.
This article is for the husbands, boyfriends, spouses, or sexual partners of anyone using a form of fertility awareness for pregnancy prevention.
Charting cycles for pregnancy prevention is a big life change, especially for the female charter. While the charter has to learn to interpret their cycles, it is fundamental that they have a supportive partner in the process.
So, What is Fertility Awareness?
Fertility awareness involves tracking one or more bio-markers of the female cycle. These bio-markers include: cervical mucus, basal body temperature, cervical position, urinary hormones, and cycle start dates. The bio-markers are used to draw a fertile window. Fertility awareness has been studied scientifically for nearly a hundred years. There are a plethora of studies on the topic. Click here to read the 2018 Overview of FABMs. In general, you can expect approximately 98 to 99% efficacy across all modern fertility awareness methods.
Your partner will be tracking based on whatever method she chooses. A method is a way of categorizing bio-markers. For example, I teach the Billings Ovulation Method. This method tracks the bio-marker cervical mucus along with sensation felt at the vulva.
One of the first things you will learn when charting is that MALES ARE FERTILE 24/7. Females are fertile only cyclically, and on average the fertile window will be for less than 1/3rd of the female menstrual cycle.
In the beginning, there is sometimes a steep learning curve with tracking these signs. Your partner may forget to check cervical mucus at every restroom break or they may be erratic in taking their temperatures. Your role at this time is be supportive. If you are living with your partner, you can help remind her to take her temperature upon first waking (if they are choosing to chart this sign!) You may also want to take part in keeping the chart.
While it is relatively rare for the partner to help chart, it is encouraged that you learn how to help classify her fertility signs or read the chart if possible. In the very least, you need to learn to respect your partner’s fertile window and not expect to ejaculate inside the vagina in the fertile window. I’m being blunt here. You will get used to “TMI” with charting! You can learn to understand the cycle by taking a class together. This is a great activity for bonding, and so that you have more equal responsibility in your family planning.
An easy way to get involved in your partner’s charting routine is to use a paper chart. I keep a paper chart on the bedside table. It is always visible. My chart is pretty easy for my partner to read because the “baby” symbols mean possible fertility. You could do this with any method. Sit down together when you record the observations. Have your partner to explain what the fertility status of the day means.
This is an example of a paper chart on heavier cardstock. The days with babies are possibly fertile. Other days are available to use when the rules allow it. Charting on paper is a great way to share your chart with ease.
But Why Would I Attend a Class or Learn About Charting if I’m NOT the Female Partner?
Because you want to be a good, supportive partner!
When you understand your partner’s chart, you understand the chance of pregnancy that you both have. This can prevent mistakes from occurring if there is more than one set of eyes on the chart. When you become attuned to your partner’s menstrual cycle, you will also begin to realize why their mood might change throughout the cycle. This is fantastic for relationship communication. Your partner is not perfect. They may make mistakes when charting. Two is better than one for catching these!!
How Will We Avoid Pregnancy in the Fertile Window?
One of the first things you will learn when reading a fertility awareness book or taking a class is that you are expected to abstain from penis-in-vagina sex in the fertile window.
The reason for this is simple: it is only possible to get pregnant in the fertile window.
If you have penis-in-vagina sex in the fertile window, there will always be a chance of pregnancy. If you are avoiding pregnancy, this means that sex in the fertile window could result in an unintended pregnancy.
During this time, it is suggested that the couple work on other aspects of the relationship. Go on dates, cuddle, talk, play games.
If you decide to break the rules by having sex, you should be prepared for the possibility of pregnancy.
For Catholics, this is the only “licit” option for the fertile window.
For non-Catholics, oral sex and sex involving hands is safe in the fertile window as long as no semen ever gets near the vulva or the vagina. If semen touches this area, pregnancy can occur.
To determine how you will proceed in the fertile window, you and your partner should place yourself on the intentions scale. In the context of fertility awareness, intentions means how open you are to pregnancy.
The basic possible intentions follow. Select which is most appropriate to you as a couple. TTA means “Trying to Avoid” a Pregnancy.
TTA Seriously Avoiding: For these people, an unintended pregnancy may be devastating, whether to health, the relationship, or finances. A pregnancy is being avoided very strictly. These people should adhere to the rules of their method as closely as possible.
TTA Regular Avoiding: For these people, pregnancy is being avoided and the rules are followed. A pregnancy wouldn’t be convenient, but it would not endanger their life.
TTA Loosely Avoiding: For these people, a broken rule isn’t the end of the world. They may do strategic risk-taking like breaking rules on the cusp of the fertile window, or using something like the withdrawal method in the fertile window. They are not actively seeking a pregnancy, but they are okay with some chance of it happening.
TTW Whatever Happens: For these people, pregnancy would be okay whenever it happens. They break whatever rules they want. They aren’t actively timing sex for the most fertile days, but it might happen.
TTCTrying to Conceive: For these people, the rules do not have to be followed. They actively try to have sex in the fertile window.
You and your partner should discuss this scale and decide where you land before utilizing the fertility awareness method for sex.
What If We Decide to Use Barriers in the Fertile Window?
Remember, while you are fertile 24/7, your female partner is not. It is really important that if you are avoiding pregnancy that you respect your partner’s fertile window.
Some couples decide to use condoms, the withdrawal method, or diaphragms in the fertile window.
The most likely time for a barrier to fail is in your fertile window. After all, you aren’t using them at the other times of the cycle.
I personally believe that a couple has the right to make an informed choice in the fertile window. In particular, the male partner should realize that he is the one putting on the condom or pulling out. If he fails to do either correctly, a pregnancy can result. If you use these methods, do the research and inform yourself about how to use them correctly and what their efficacy is. If you are okay with this risk, you can use barrier methods. At the point you use a barrier method – you are outside of correct use for the fertility awareness method. Always remember that. An unintended pregnancy would be classified as a user error or barrier method failure.
How Long Does it Take to Practice Fertility Awareness Confidently?
On average, you will want to do at least 3 to 6 cycles of follow-up with an instructor to be completely autonomous and confident in charting. When you work with an instructor, you may be able to start utilizing the method to avoid pregnancy as sooln as the first cycle charting! (This is assuming that your partner has been diligent in their charting).
If you have PCOS, are coming off hormonal birth control, or are breastfeeding, you may need close instruction for longer. The Billings Ovulation Method recommends following up until the third ovulatory cycle postpartum. This could take a year or more if fully breastfeeding.
To Male Partners:What Advice Would You Give Male Partners Who Are New To Fertility Awareness?
These responses are taken from a 2019 survey I did on the male partners of FAM users. Enjoy!
“At first it seems backwards since science has a simple fix for conception: hormonal birth control. Some women are fine on hormonal birth control. Some can be really crazy on it. With some women, it can even kill their sex drive. With mine, she becomes so crazy that it kills both of our sex drives. So we’re doing this weird fertility awareness thing. Here’s my advice if you have a woman like mine. Even though she’s so beautiful and sexy that you just want to risk ejaculating in her to possibly get her off, you can’t do it with this. Yes, it puts more pressure on you to wear a condom and/or pull out, but at least your wife isn’t batshit crazy. And she’s still horny. So it’s worth it. Plus you learn a lot about the female body because I guarantee she’ll keep you up at night telling you about it lol. So don’t complain. We’re still getting laid. Unlike our friends who’s wives are on the pill or IUD. It just puts more pressure on us to prevent a baby. If she gets pregnant again, it’s probably our fault with this. And I’m ok with that. War Eagle!”
“You will wish you had always known this information. Test your pre-cum under a microscope for sperm if you are going to use withdrawal.”
“Knowledge is power and pleasure.”
“To do the research to fully understand the anatomy and physiology which will give you confidence in trusting the fertility awareness method.”
“Good luck m’a friend.”
“Embrace it.”
“Don’t be afraid to ask questions!”
“Be patient and understanding whilst always at least attempting to understand the technicalities surrounding the practice of the method.”
“Listen.”
“Read as much information as you can and stay informed.”
“Trust your partner, but do some cursory research as well. You both need to understand it to trust it.”
“Learn the actual science (as in the research literature) behind these technologies. Much of the medical establishment unfortunately has both insufficient and badly-outdated knowledge about FAM. Also, such will only be successful if the couple are both wholly on-board and possess the necessary knowledge, discipline, and self-control to utilize the method(s) correctly, whether trying to conceive or to avoid.”
“Get ya woman on it like yesterday.”
“Talk to your significant other and learn from her.”
“Learn about which days are the best to get pregnant; if you want to get pregnant together there is a way to learn the best days with a good degree of certainty. I think other men could benefit from learning this information about their partner.”
“Learn how the world works, and use that knowledge.”
“Listen to your woman and trust what she says about her observations. It’s not like the guy is the one using the method, but it’s good to be aware of it.”
“If you think it’s burdensome, remember the health and relationship benefits far outweigh the daily minor inconveniences. Encourage your SO to do the research to make sure they’re doing it right as well.”
“Shut up, pay attention.”
“If you are concerned about the well being of your partner, you’re more likely to succeed in supporting her and have an involved role in fulfilling both your reproductive goals through fertility awareness.”
“Be patient.”
“Take a lesson yourself or attend one with your partner, you are only going to trust it if you understand how it works yourself. When you actually see that it makes sense, it’s not some weird alternative thing, you can trust it a lot more.”
This resource is a simple overview of the rules with examples. It links to other resources on understanding the female and male reproductive system. This is a good, fairly quick read for men who want to understand the basic rules.
Jessie discusses her symptoms that lead her to stop taking hormonal birth control. She then does a brief overview of how the fertility signs change throughout the cycle and how sperm life plays into fertility.
This also leans religious but may be useful for men who are having trouble adjusting to avoiding unprotected sex in the fertile window.
“Use of Natural Family Planning (NFP) and Its Effect on Couple Relationships and Sexual Satisfaction: A Multi-Country Survey of NFP Users from US and Europe.” Front Public Health. 2017; 5: 42. Published online 2017 Mar 13. doi: 10.3389/fpubh.2017.00042
This is a recent scientific article that studied the effect of NFP on relationships.
I purchased a Fitbit device close to two years ago, and within months I noticed that my heart rate appeared to be correlating with the phases of my cycle. I’ve been charting resting heart rate since 2018, and I can say with confidence that it has lined up every cycle. This shouldn’t be too surprising because we already know that progesterone causes basal body temperature to rise, but heart rate does not exactly follow that pattern. Heart Rate also rises in response to high estrogen levels in the fertile window.
We have known about the possible connection between heart rate and the menstrual cycle for over a century, but in the last 50 years a few studies have taken a closer look.
Palmero (1991) studied 64 women for 3 consecutive months and created a PMS group versus a non-PMS group. They found that “in the premenstrual phase, PMS group showed significantly higher resting HR levels than NPMS group.”
Moran (2000) followed 26 women and found that “resting-heart rate was significantly higher in both ovulatory (P < 0.01) and luteal (P < 0.01) phases than in the menstrual and follicular phases.”
Shilaih (2017) followed 91 women and found that they “observed a significant increase in pulse rate (PR) during the fertile window compared to the menstrual phase (2.1 beat-per-minute, p < 0.01). Moreover, PR during the mid-luteal phase was also significantly elevated compared to the fertile window (1.8 beat-per-minute, p < 0.01), and the menstrual phase (3.8 beat-per-minute, p < 0.01).”
I want to highlight these last two studies in particular, because many of the other studies have an issue. Marco Altino explains why:
“The great majority of studies looking at HRV and the menstrual cycle collected one single data point during the follicular phase and one single data point during the luteal phase. I don’t have to tell you how little sense that makes, considering the high day to day variability in these parameters.”
This is an excerpt from his blog on heart rate variability in the menstrual cycle. Read the full blog here.
The 2017 study published in Nature by Shilaih, et al found that heart rate may rise up to 5 days before ovulation occurs. This means that heart rate could potentially be a used as a way to time intercourse for conception.
My results are so steady with resting heart rate that I dream of someone using it in a long-term study with other fertility signs. Wouldn’t it be cool if we could avoid pregnancy using heart rate too?
Below is an example of my results with resting heart rate. To convert my heart rate to fit in a fertility awareness app, I use a conversion. Essentially, one heart rate beat = .1 Farenheit change on my temperature scale. A heartbeat of 69 becomes 96.9, 70 becomes 97.0, 71 becomes 97.1 This preserves the original ratio, and it allows me to show the data with other fertility signs. For your own conversion, you may model this. If you have a lower heart beat rate, you can still convert, but you may need to do an additional equation.
My resting heart rate rose during the most fertile days of the cycle. Ovulation most likely occured on Cycle Day 15 or Cycle Day 16 on this chart. In addition, while I have not found evidence of this in the literature, I have observed that I tend to get a one day rise 3 to 4 days before the fertile window opens with cervical mucus. On this chart, that was Cycle Day 6. A second example. Ovulation most likely occured on Cycle Day 14, 15 or 16. Heart rate rose on Cycle Day 14.
In conclusion, I believe that resting heart rate is a very unique sign to track, especially if you already use a wearable fitness tracker. I will note that a false heart rate rise can be caused by illness, alcohol or food close to bedtime, nightmares, and more! This is not dissimilar to what can obscure a temperature. I hope that in the future more studies are done so that we can see if heart rate can also be used for avoiding pregnancy purposes.
Selected Heart Rate Study Citations
Moran, V. H., Leathard, H. L., & Coley, J. (2000). Cardiovascular functioning during the menstrual cycle. Clinical physiology (Oxford, England), 20(6), 496–504. https://doi.org/10.1046/j.1365-2281.2000.00285.x
Palmero, F., Choliz, M. Resting heart rate (HR) in women with and without premenstrual symptoms (PMS). J Behav Med14, 125–139 (1991). https://doi.org/10.1007/BF00846175
Shilaih, M., Clerck, V., Falco, L. et al. Pulse Rate Measurement During Sleep Using Wearable Sensors, and its Correlation with the Menstrual Cycle Phases, A Prospective Observational Study. Sci Rep7, 1294 (2017). https://doi.org/10.1038/s41598-017-01433-9





























You must be logged in to post a comment.