
Many people think that having sex during menstruation cannot lead to pregnancy, but the answer is much more nuanced than that. It is possible to get pregnant during bleeding episodes, some of which may not be menstruation!
Was the bleeding truly menstruation?
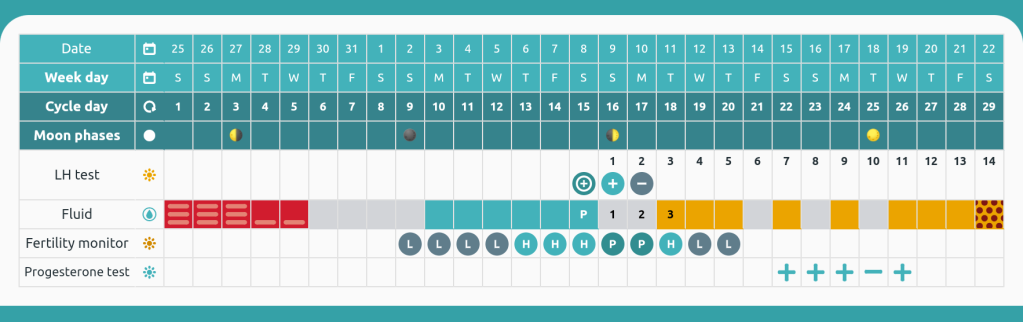
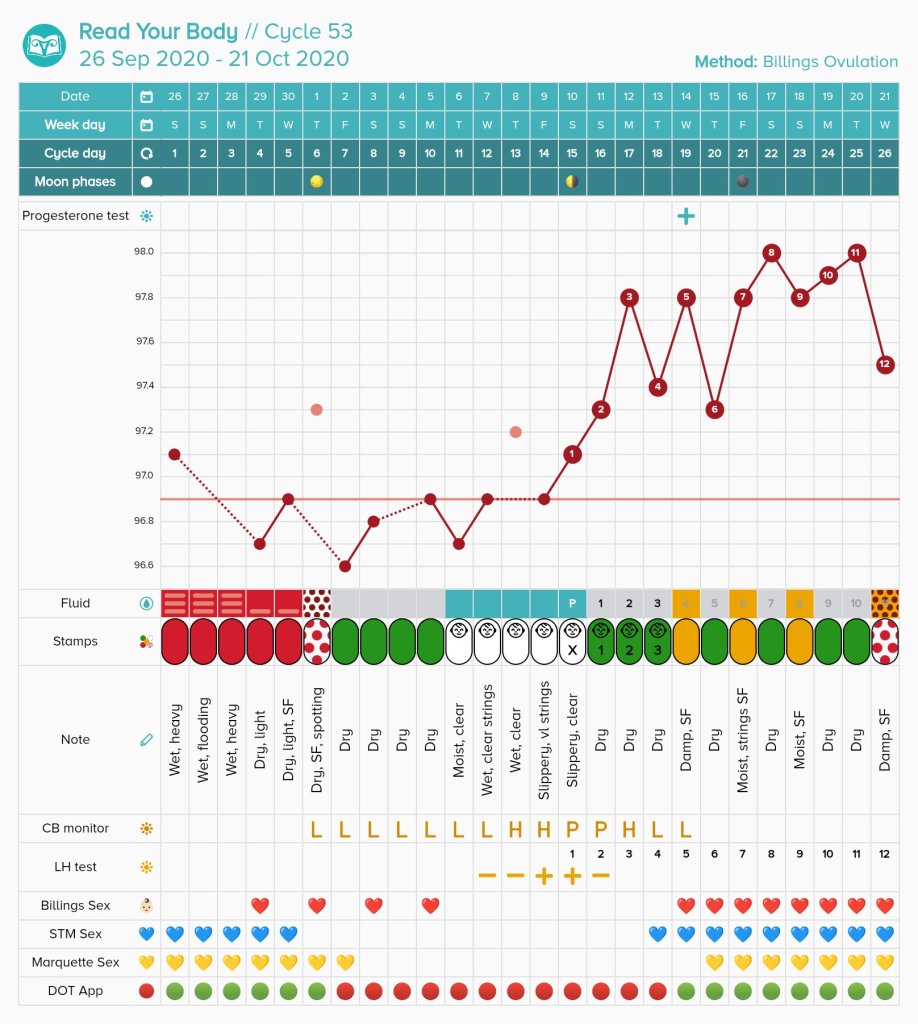
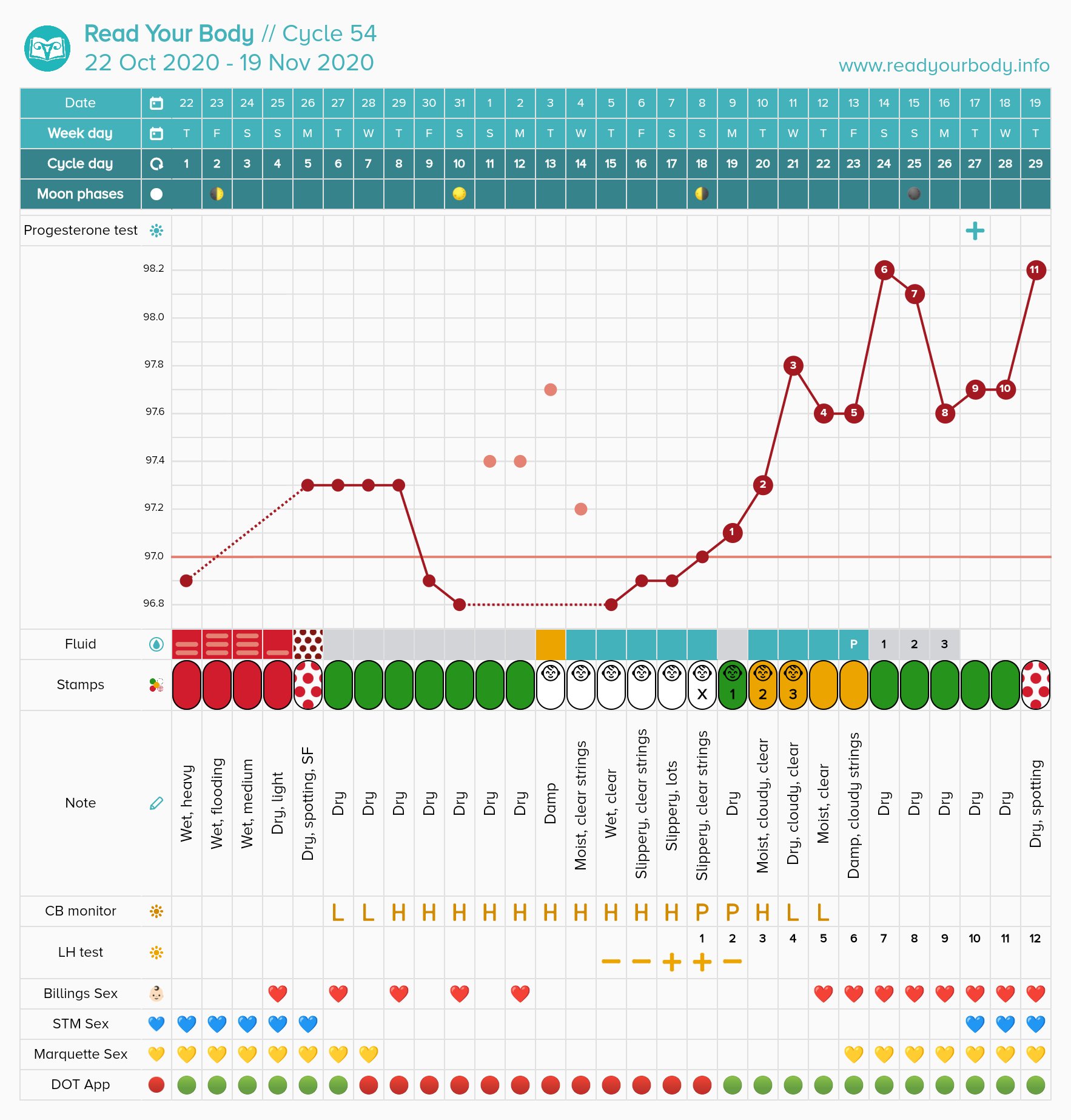
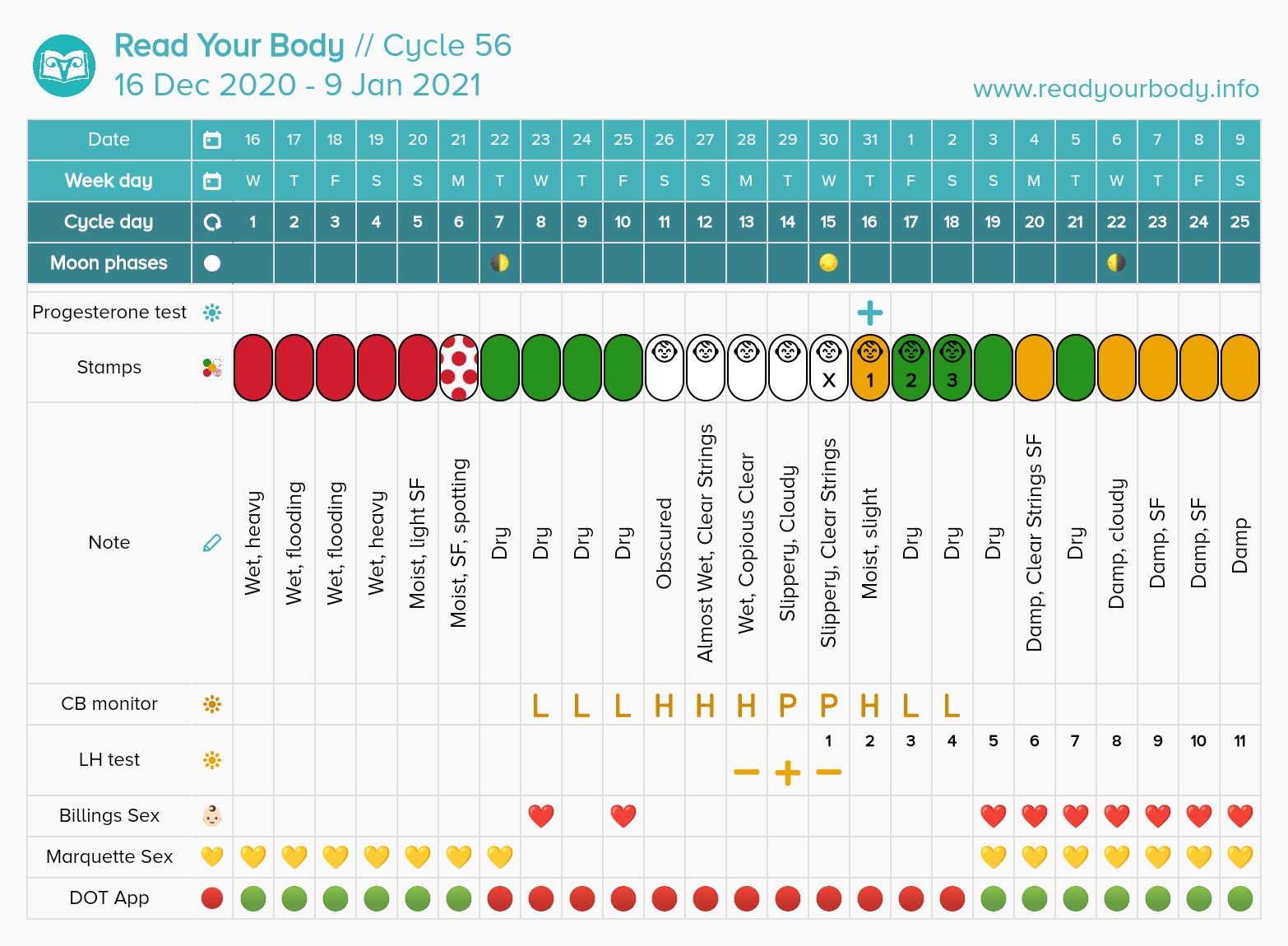
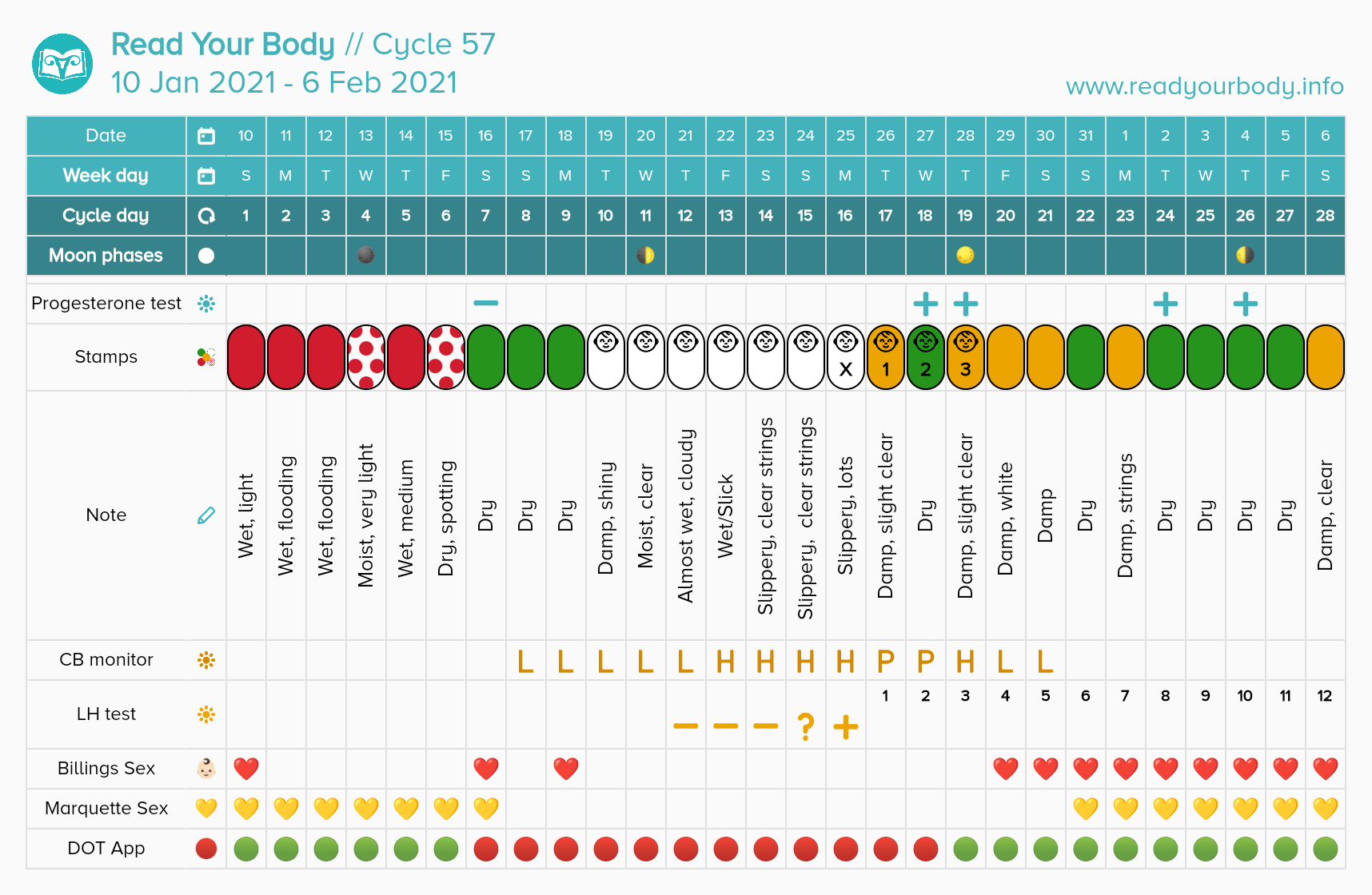
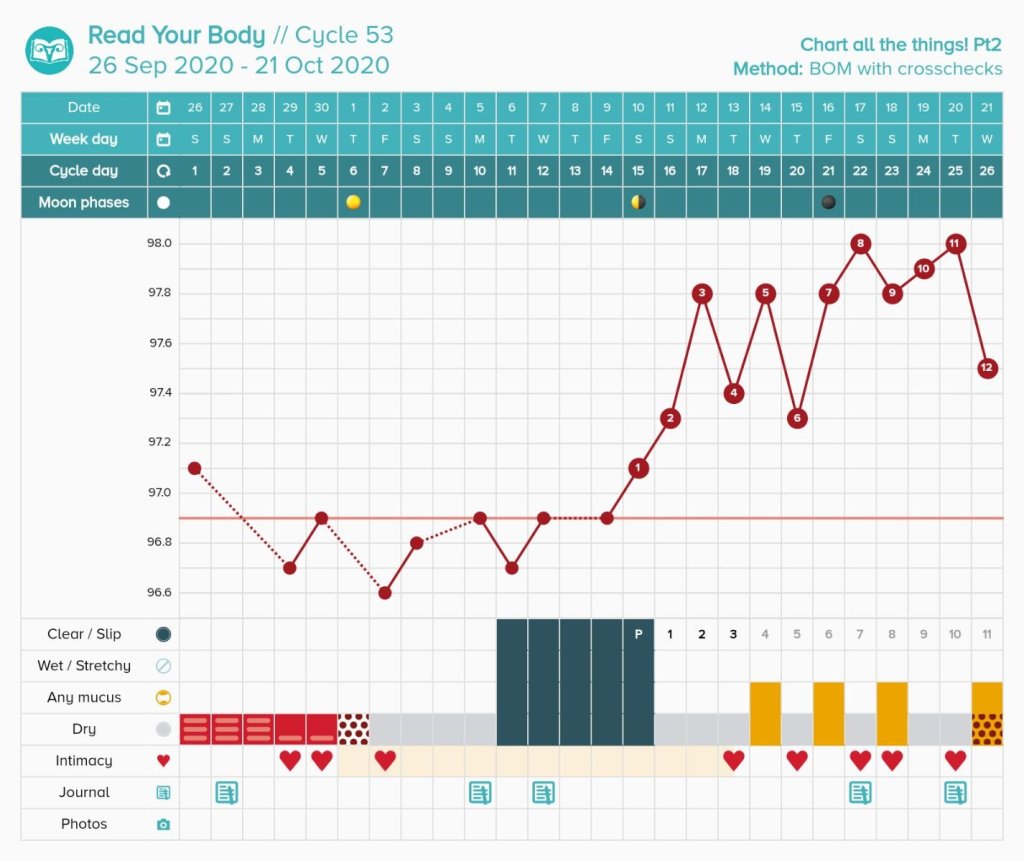
Charting evidence-based fertility signs like cervical mucus, basal body temperature, and urinary tests are the best way to determine if you are ovulating. True menstruation should follow about 10-16 days post ovulation as indicated by a temperature shift or positive PdG test.
If you are not charting your cycle with a fertility awareness based method, your bleeding may not really be menstruation. Estrogen breakthrough bleeding may appear very similar to menstruation and is often indistinguishable without charting. This bleeding can be fertile, and pregnancy could result.
Day one of a true menstruation marks the beginning of the cycle.
How long are your cycles? Better yet, approximately when do you usually ovulate?
If your cycles were 26 days or longer for the last year, it is unlikely you will become pregnant with sex during the first five days of the cycle.
Dr. Josef Roetzer monitored 5,807 cycles. He observed only one pregnancy before day 6 of the cycle. Her cycles were 22-27 days long.
Dr. Roetzer estimates that using the first five/six days is 99.8% effective for avoiding pregnancy. It is important to note that all of his cycles monitored had a temperature shift preceding menstruation. If you do not have proof that you ovulated before a bleed, it becomes more likely to conceive during bleeding.
Another way to determine the last infertile day at the beginning of the cycle is to use Dr. Doering’s rule. Dr. Doering subtracted 7 from the earliest first high temperature in the last year. For example, Sarah’s earliest first high temperature was day 13. Day 13 – 7 = Day 6 as the last infertile day of the cycle. This rule is always crosschecked with cervical mucus. Sperm may survive up to 5 days in cervical mucus, and any presence that has not been determined to be infertile through instruction should open the fertile window. The Doering rule is more personalized than automatically assuming the first five/six days are infertile.
In Dr. Frank-Hermann’s double-check sympto-thermal study from 2007, all three method failures were from day 5 intercourse. This study used the first five day rule and Doering rule. This study yielded an efficacy of 99.6%.
So am I safe to have sex during my period? Ask yourself these questions.
- Did you confirm ovulation with basal body temperature, PdG strips, or a blood draw in the previous cycle?
- Are your cycles longer than 26 days on average? Have you ever had a peak day before day 13 of the cycle?
If the answer to both of those is yes, you can probably have safe sex up to day 5 of your cycle.
If your answer is no, then you have a possibility of pregnancy.
What if I want to be more conservative?
Some methods like Billings, FEMM, and Creighton suggest not having sex during heavy days of bleeding when cervical mucus cannot be observed.
If you have a history of short cycles (less than 26 days) or want to add an extra layer of protection onto the beginning of the cycle, I recommend beginning observing vulva sensation and cervical mucus as soon as your bleeding has lightened enough to no longer need a tampon, cup, or regular pad. If you need only a panty liner or are only experiencing light spotting, you should beginning checking your cervical mucus and sensation throughout the day. At the end of your day, if you have observed no cervical mucus or sensation outside of your determined infertile pattern, this day is safe for sex. (DO NOT DO THIS WITHOUT LEARNING A METHOD. THIS BLOG IS NOT ENOUGH INFORMATION TO AVOID PREGNANCY WITH ALONE).
What if I bleed for more than 5 days?
If your menstruation lasts longer than five days, you should follow the instructions from the paragraph above. It is NOT safe to consider past day 5 automatically available if you are bleeding. You need proof by using cervical mucus or urinary estrogen tests that your fertile window has not yet opened past day 5 of the cycle.
What if I randomly have a short cycle?
Checking cervical mucus is your best back up. Cervical mucus should appear when the fertile window is opening for most charters. Many methods suggest no longer considering menstruation safe once you enter peri-menopause (can occur up to 10 years before menopause) because cycles may shorten at this time. If you notice that your cycles have grown shorter than 26 days, you may want to become more vigilant and stop automatically considering the first 5 days safe.
Conclusion
For the majority of people menstruating, using the first five days of a true menstrual cycle will not result in pregnancy. For a very small percentage, it may. I recommend charting with a real fertility awareness method (Sensiplan, SymptoPro, FEMM, Billings, Marquette, etc) to determine if your bleeding is actually menstruation!
Works Cited
Roetzer, Josef. “Further Evolution of the Sympto-Thermal Methods.” International Review of Natural Family Planning 1 (1977): 139-150.
Raith-Paula, Elisabeth, et al. Natürliche Familienplanung heute. Springer Medizin Verlag Heidelberg, 2008.
















































You must be logged in to post a comment.