During the postpartum period of time, fertility is in a unique state. For those fully breastfeeding, it may be months or years before they begin ovulating again regularly and with fertile cycles. This article talks about some of the data we have on what return of fertility looks like. This information may be of particular interest to those charting with a method of natural family planning or fertility awareness. Charting at this time may be difficult, and for highest efficacy should be done closely with a certified natural family planning educator.
Breastfeeding as Birth Control
Breastfeeding has been shown over numerous studies to have an effect on return to fertility and ovulation. Kennedy et al (1989) reviewed 10 studies from multiple countries to come to a consensus on what full-breastfeeding means.
- Fully breastfeeding or at least partially fully breastfeeding
- Fully breastfeeding meaning the infant gets all or as close to all as possible of their nutrition by suckling at the breast directly, no bottles or pumping
- Small bites of regular food or water do not disqualify for full breastfeeding
- No bleeding past day 56 postpartum until the 6 month mark postpartum.
Some methods suggest going no longer than 6 hours at night without breastfeeding. While this was not mentioned in the study, it is generally used as the standard in fertility awareness based methods to see if someone qualifies to rely on the lactational amenorrhea method (LAM).
LAM is 98% effective for avoiding pregnancy when all criteria is met up until 6 months postpartum. After that, efficacy drops precipitously.
What about ecological breastfeeding?
Ecological breastfeeding requires even stricter criteria and may delay fertility for much longer. Bleeding past day 56 does not disqualify someone for ecological breastfeeding. Ecological breastfeeding should not be confused with LAM! Ecological breastfeeding was coined by Dr. Sheila Kippley. You can buy her book here.
The criteria include:
- Breastfeed exclusively for 6 months
- Pacify your baby at your breast
- No bottles or pacifiers
- Sleep with your baby for night feedings
- Sleep with your baby for a daily-nap feeding
- Nurse frequently day & night. Avoid schedules.
- Avoid anything that would separate you from your baby / prevent regular nursing
Symptothermal Method Studies on Breastfeeding
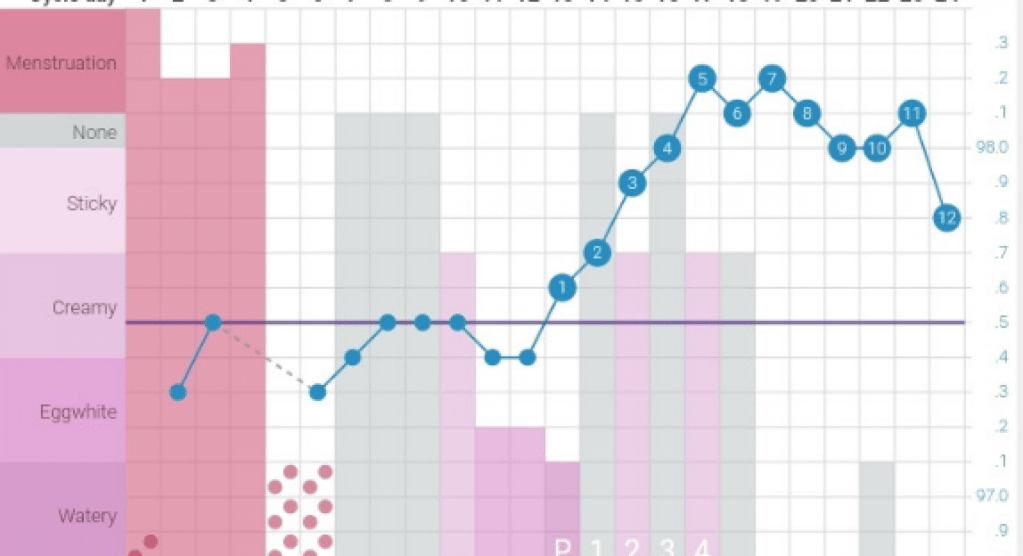
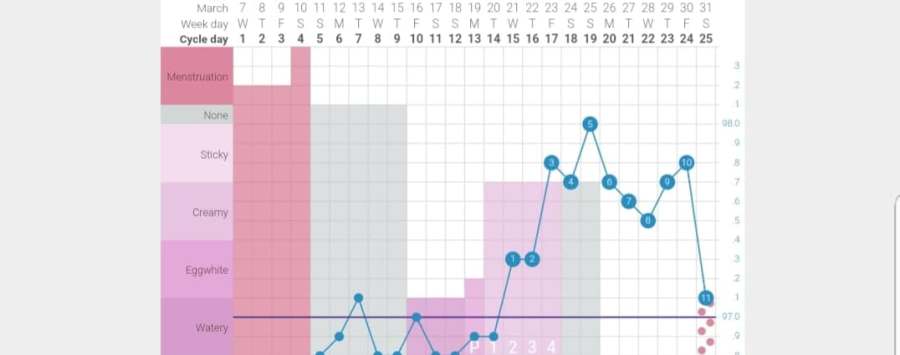
For the first part of this overview, I am going to cover a few symptothermal studies that followed breastfeeders from birth to return of fertility. Symptothermal charters record cervical mucus and basal body temperature daily in order to track their fertility and determine when the fertile window is opened and when it is closed.
In “Breastfeeding and the Symptothermal Method,” Kennedy et al. followed 73 women who charted with a symptothermal method in Australia, Canada, England. While this is a small sample size, the team collected a ton of data: 22,538 diary sheets, 9,428 urinary vials to measure hormones, and 1,600 follow-ups with the women (Kennedy 1995).
Kennedy et al. reported the following data regarding the wait to return of fertility:
- Only 25% of first ovulations postpartum had “adequate luteinization.” This means over three quarters of first ovulations were likely infertile (Kennedy, 110).
- In retrospect, up to 51% of possibly fertile days identified by sympto-thermal would not have lead to conception (Kennedy, 112). The study standard for this was 5 day sperm life.
- They found that 94-99% of the time, the sympto-thermal method correctly identified when a day was really infertile. This means that around 1-6% of the time it didn’t identify a day that may have lead to pregnancy (Kennedy, 112).
- They recorded four adequate ovulations with those fully breastfeeding for their first ovulation. This was defined as a 10 day or greater luteal phase with adequate progesterone levels. (Kennedy, 112).
- Abstinence was expected per the rules for about 50% of the charted days included in the study (Kennedy, 113).
Bonus Information for Cervical Mucus Fans: Fertile mucus in this study was considered anything cloudy, opague, clear, translucent, stretchy, strands, wet, lubricative, moist, or unusually abundant.
Zinaman and Stevenson in the USA followed 25 women until they had 3 ovulatory cycles postpartum (1991).
They found the following data regarding return to fertility:
- 20% of ovulations in the first ovulation postpartum during the first 6 months were considered fertile (ie a luteal phase longer than 10 days) (Zinaman and Stevenson, 2037).
- Basal body temperature appeared inadequate to capture the first ovulation, occurring up to 4 days after the LH peak, but it improved in later cycles (Zinaman and Stevenson, 2037).
| Percentage | Time to Return of Fertility From Birth |
| 25% | Less than 200 days |
| 25% | 200 to 300 days |
| 35% | 301 to 400 days |
| 15% | More than 400 days |
In an article in the International Review of Natural Family Planning, Parenteau-Carreau presents data collected from 43 postpartum women charting with the Serena Canada method.
Parentau-Carreau reports the following data on postpartum charting:
- 65% of first bleeds were preceded by a thermal shift (35).
- The collection of charts confirmed the theory that 4 high temperatures should be used postpartum, as there were instances of 3 raised temperatures that were not true shifts (36).
- Among temperature shifts during the first 6 months postpartum, 75% lasted 8 days or more (37).
- For babies who sucked their thumb or used a pacifier regularly, their mothers experienced return of fertility an average of 13 days earlier than those who only breastfed for soothing purposes (37).
- The basal body temperature curve tended to become more steady or regular in the one to two weeks prior to the first ovulation (38).
What can we conclude from all this data?
- Breastfeeding and meeting the criteria for LAM is highly effective for avoiding pregnancy in the first 6 months postpartum.
- Most first ovulations postpartum are infertile (defined as a luteal phase less than 10 days long).
- It is possible to chart during postpartum to avoid pregnancy.
What methods work best postpartum?
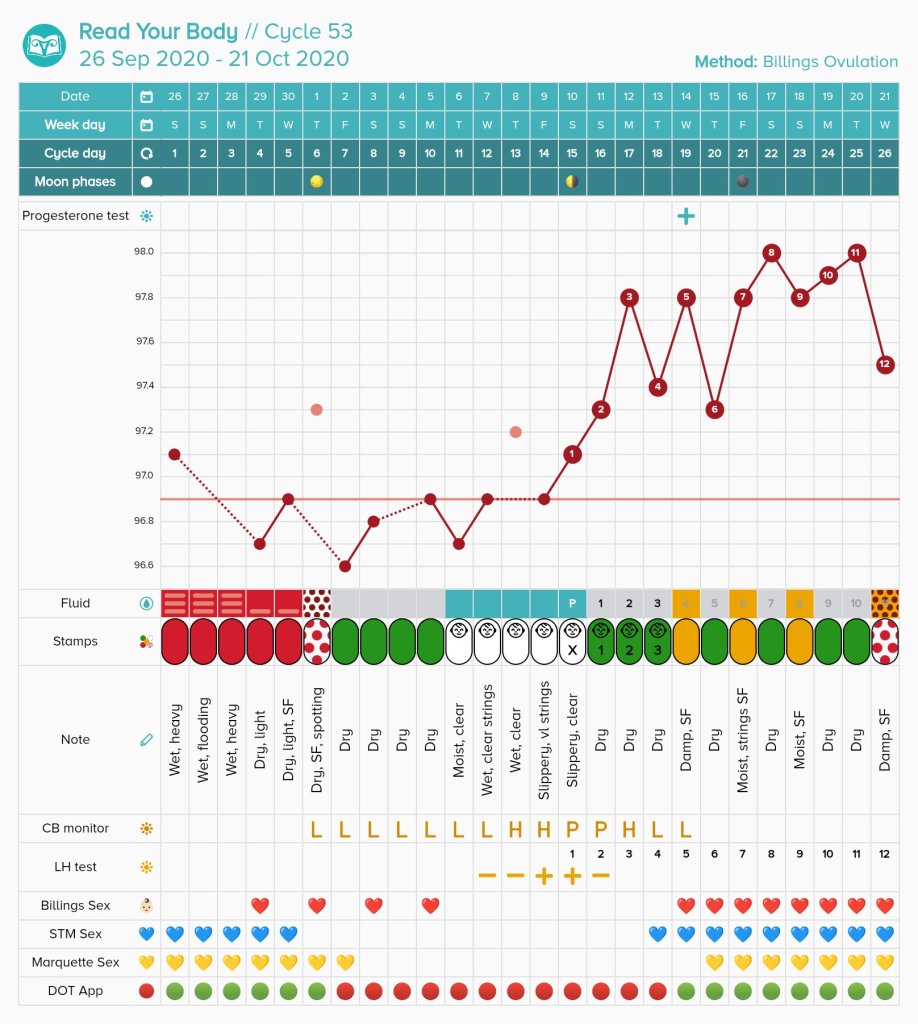
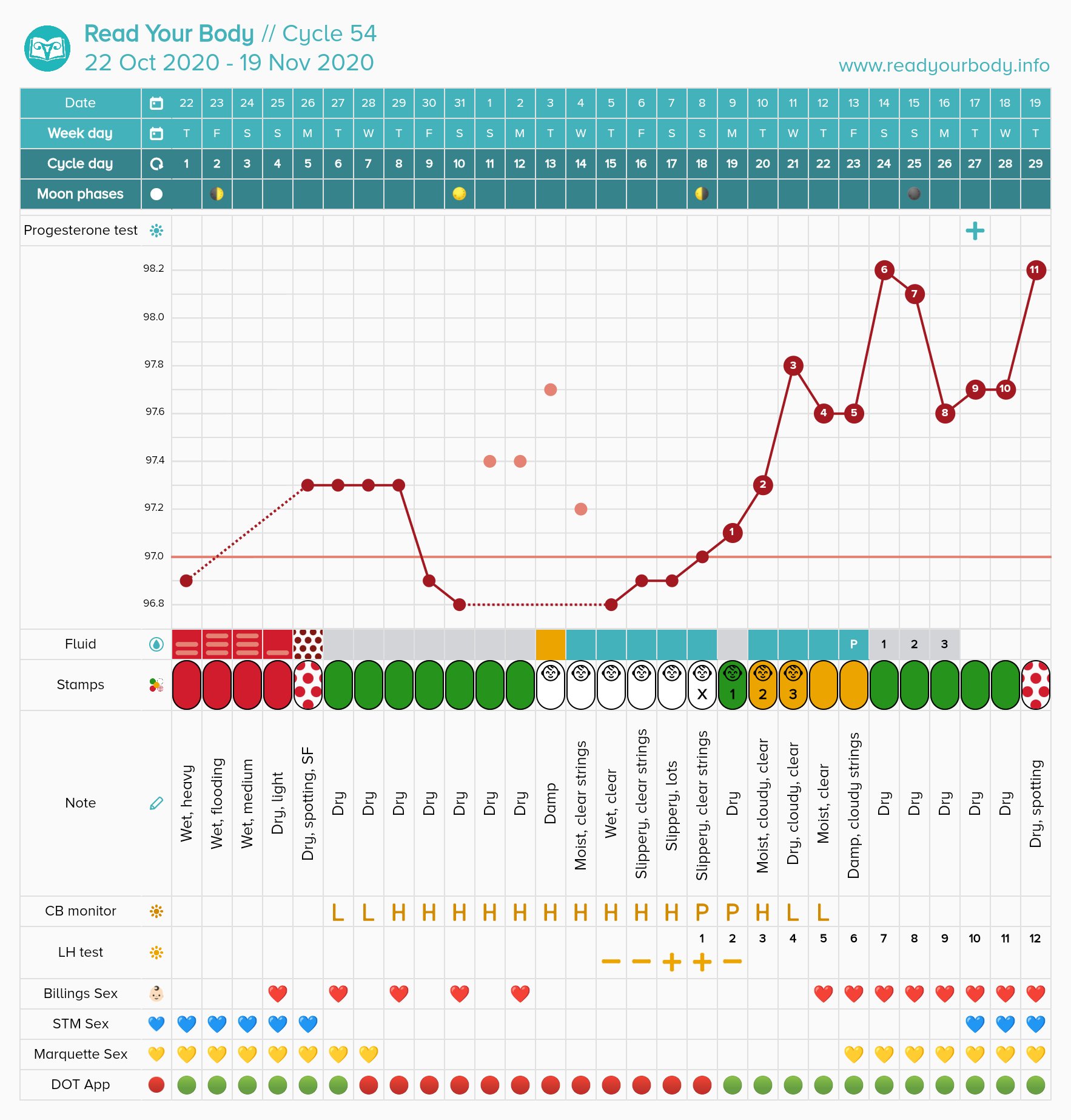
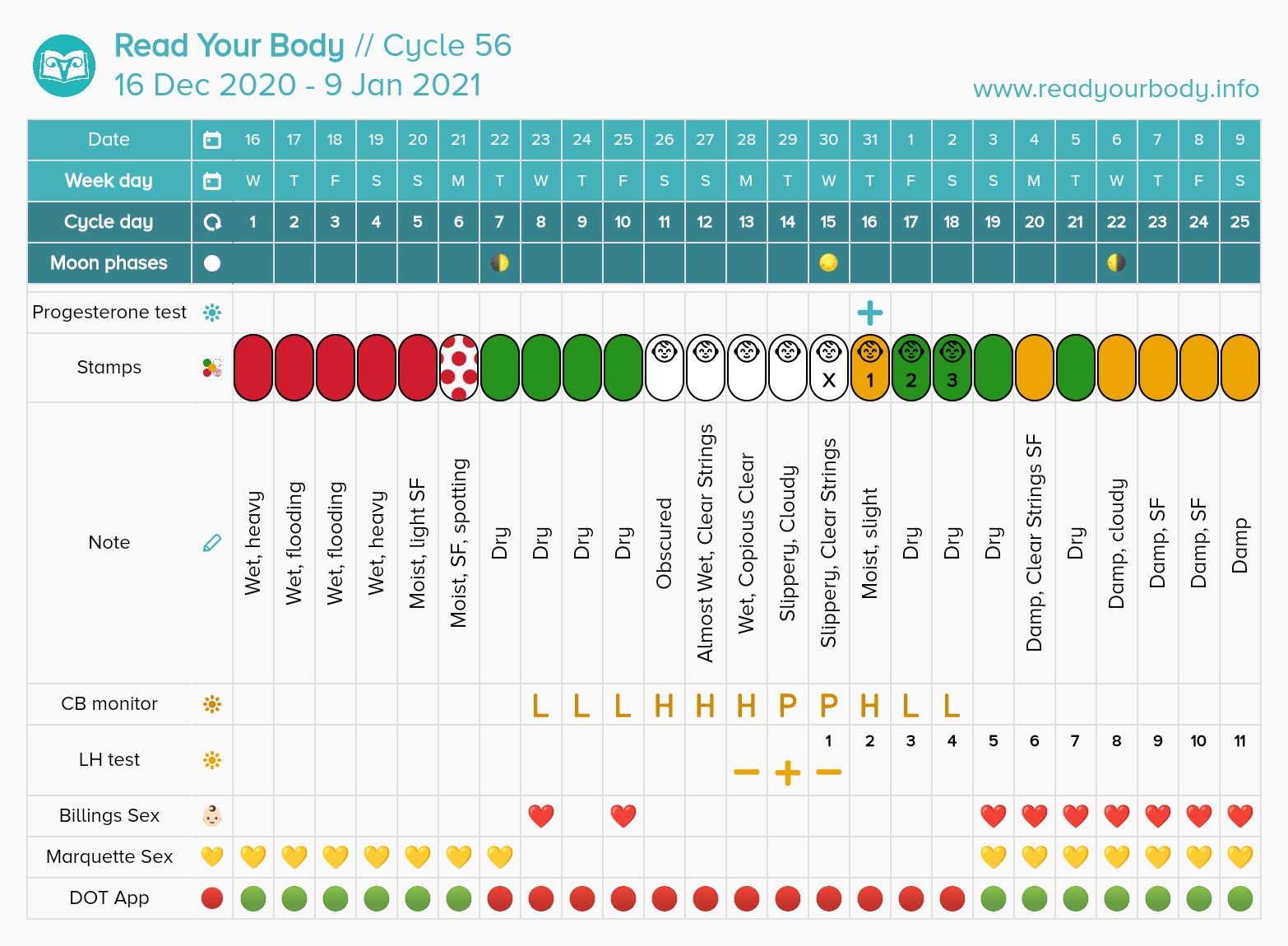
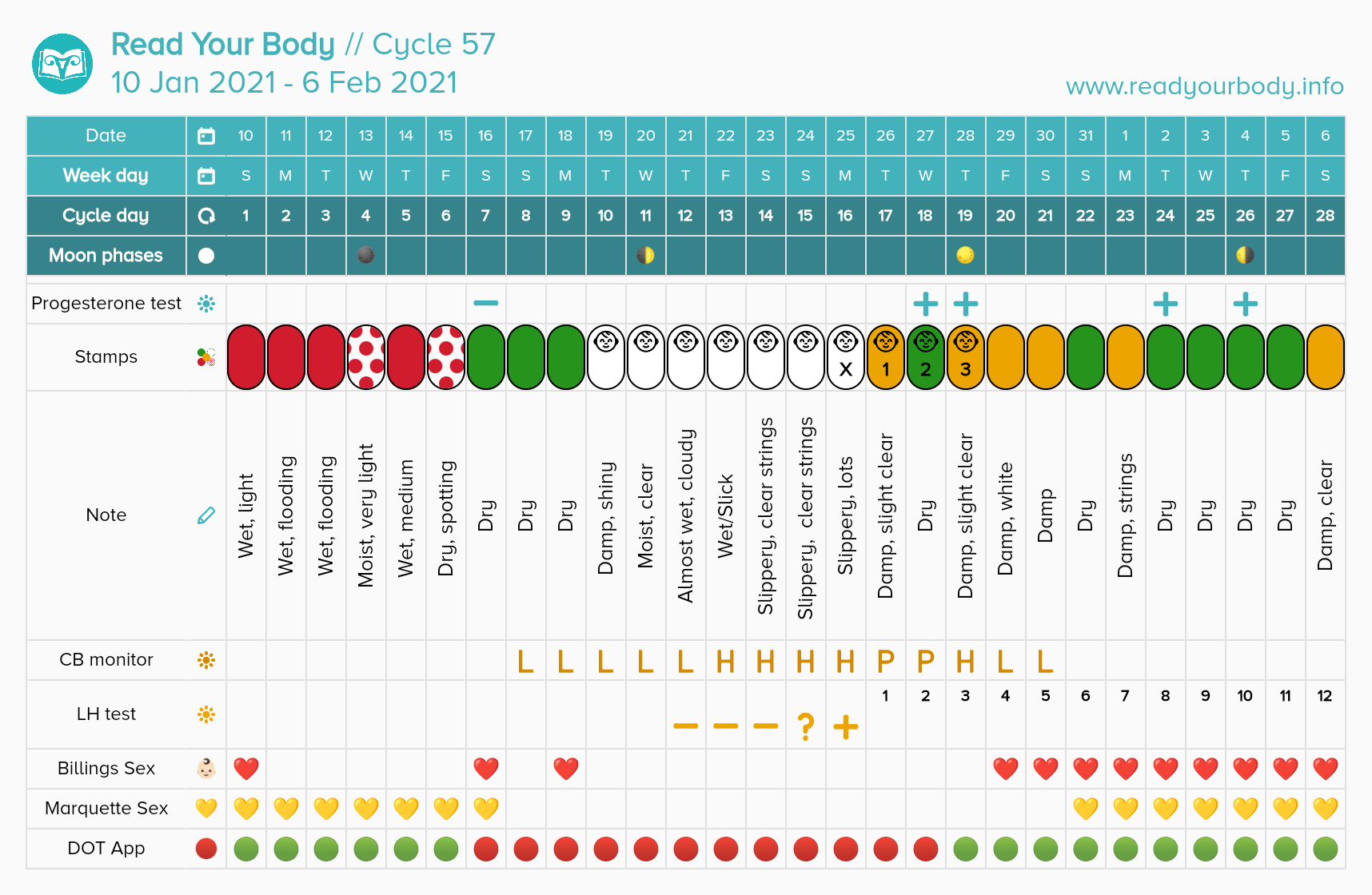
I recommend practicing either the Billings Ovulation Method or Marquette postpartum. I do not recommend sympto-thermal method because temperatures are not useful until fertility returns. I only recommend taking your temperature before the 6 month mark to those who are not breastfeeding. In addition, the sympto-thermal method offers less complex mucus patterns than Billings does.
Billings Ovulation Method involves charting sensation at the vulva and appearance of mucus to create a basic infertile pattern. It allows only alternate evenings of the basic infertile pattern for sex until return of fertility (IE ovulation) occurs. It is approximately 98% effective with correct use postpartum.
- Subjective fertility signs (sensation and appearance)
- Only alternate evenings for sex
- Very affordable (Billings will work to set you up with a free instructor if you absolutely cannot afford one)
- No re-occurring cost
- One-time cost for instruction (ideally, please pay your educator if you can! Some instructors may charge after 1-2 years pass)
Marquette Method involves charting urinary hormones using the Clearblue monitor. This monitor reads estrogen and LH levels. This method is going to be more expensive than a cervical mucus only method, so I only recommend it to those who can afford approximately $30 USD a month or more postpartum. Unfortunately, the stick costs fluctuate up to $50 USD or so for 30 sticks, but I have seen them as low as $30 USD. Marquette is approximately 98% effective with correct use.
- Objective fertility signs (monitor does the reading for you)
- Any time of day sex when available
- Expensive by some standards. Sticks cost twice as much in Europe. May not be available in some countries at all.
- Re-occurring cost
- One-time cost of the monitor ($50-$130 USD depending on if buying new or used)
- One-time cost of instruction (unless you go over the year mark, you may need to pay twice)
- I have heard that some instructors may offer scholarships, but you would need to contact individual instructors or organizations to learn their policies.
References
Kennedy, K; Rivera, R; McNeilly, A. (1989). Consensus statement on the use of breastfeeding as a family planning method. , 39(5), 0–496. doi:10.1016/0010-7824(89)90103-0
Kennedy, K., Gross, B., Parenteau-Carreau, S., Flynn, A., Brown, J., & Visness, C. (1995). “Breastfeeding and the Symptothermal Method.” Studies in Family Planning, 26(2), 107-115. doi:10.2307/2137936
Parenteau-Carreau, S. (1984). “The Return of Fertility in Breastfeeding Women.” The International Review of Natural Family Planning. Vol. 8(1). pp. 34-38.
Zinaman, Michael; Stevenson, Wilma (1991). Efficacy of the symptothermal method of natural family planning in lactating women after the return of menses. American Journal of Obstetrics and Gynecology, 165(6), 2037–2039. doi:10.1016/S0002-9378(11)90575-4































You must be logged in to post a comment.