
I purchased a Fitbit device close to two years ago, and within months I noticed that my heart rate appeared to be correlating with the phases of my cycle. I’ve been charting resting heart rate since 2018, and I can say with confidence that it has lined up every cycle. This shouldn’t be too surprising because we already know that progesterone causes basal body temperature to rise, but heart rate does not exactly follow that pattern. Heart Rate also rises in response to high estrogen levels in the fertile window.
We have known about the possible connection between heart rate and the menstrual cycle for over a century, but in the last 50 years a few studies have taken a closer look.
Palmero (1991) studied 64 women for 3 consecutive months and created a PMS group versus a non-PMS group. They found that “in the premenstrual phase, PMS group showed significantly higher resting HR levels than NPMS group.”
Moran (2000) followed 26 women and found that “resting-heart rate was significantly higher in both ovulatory (P < 0.01) and luteal (P < 0.01) phases than in the menstrual and follicular phases.”
Shilaih (2017) followed 91 women and found that they “observed a significant increase in pulse rate (PR) during the fertile window compared to the menstrual phase (2.1 beat-per-minute, p < 0.01). Moreover, PR during the mid-luteal phase was also significantly elevated compared to the fertile window (1.8 beat-per-minute, p < 0.01), and the menstrual phase (3.8 beat-per-minute, p < 0.01).”
I want to highlight these last two studies in particular, because many of the other studies have an issue. Marco Altino explains why:
“The great majority of studies looking at HRV and the menstrual cycle collected one single data point during the follicular phase and one single data point during the luteal phase. I don’t have to tell you how little sense that makes, considering the high day to day variability in these parameters.”
This is an excerpt from his blog on heart rate variability in the menstrual cycle. Read the full blog here.
The 2017 study published in Nature by Shilaih, et al found that heart rate may rise up to 5 days before ovulation occurs. This means that heart rate could potentially be a used as a way to time intercourse for conception.
My results are so steady with resting heart rate that I dream of someone using it in a long-term study with other fertility signs. Wouldn’t it be cool if we could avoid pregnancy using heart rate too?
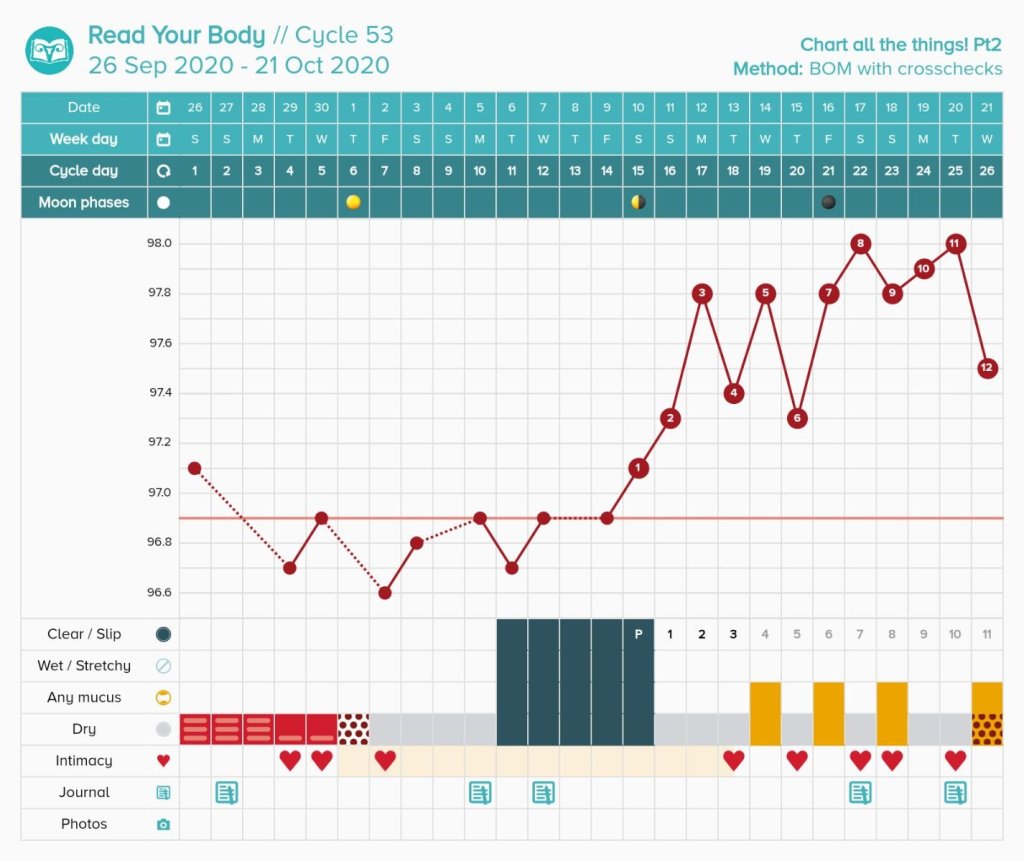
Below is an example of my results with resting heart rate. To convert my heart rate to fit in a fertility awareness app, I use a conversion. Essentially, one heart rate beat = .1 Farenheit change on my temperature scale. A heartbeat of 69 becomes 96.9, 70 becomes 97.0, 71 becomes 97.1 This preserves the original ratio, and it allows me to show the data with other fertility signs. For your own conversion, you may model this. If you have a lower heart beat rate, you can still convert, but you may need to do an additional equation.


In conclusion, I believe that resting heart rate is a very unique sign to track, especially if you already use a wearable fitness tracker. I will note that a false heart rate rise can be caused by illness, alcohol or food close to bedtime, nightmares, and more! This is not dissimilar to what can obscure a temperature. I hope that in the future more studies are done so that we can see if heart rate can also be used for avoiding pregnancy purposes.
Selected Heart Rate Study Citations
Moran, V. H., Leathard, H. L., & Coley, J. (2000). Cardiovascular functioning during the menstrual cycle. Clinical physiology (Oxford, England), 20(6), 496–504. https://doi.org/10.1046/j.1365-2281.2000.00285.x
Palmero, F., Choliz, M. Resting heart rate (HR) in women with and without premenstrual symptoms (PMS). J Behav Med 14, 125–139 (1991). https://doi.org/10.1007/BF00846175
Shilaih, M., Clerck, V., Falco, L. et al. Pulse Rate Measurement During Sleep Using Wearable Sensors, and its Correlation with the Menstrual Cycle Phases, A Prospective Observational Study. Sci Rep 7, 1294 (2017). https://doi.org/10.1038/s41598-017-01433-9








































You must be logged in to post a comment.