
I recently completed my teaching certification for the Billings Ovulation Method through the Billings Ovulation Method Association in the USA (BOMA). This is a cervical mucus / sensation only method that has been taught for over fifty years in over 120 countries.
I began this certification having been quite dissatisfied with my previous certification in the sympto-thermal method. I found the sympto-thermal method inadequate for irregular cycles or postpartum cycles, as well as for any cycles with continous mucus.
This certification 100% cleared up all doubts I had about being able to teach people in these situations! I love that Billing’s motto is “Keep it simple.” Ultimately, this certification gave me the confidence to give up temperature taking as a part of my fertility awareness routine.
First Step:
Before beginning the certification, I took an introductory class with my spouse in the method. This gave me about 6 months to try to apply the principles to my charts before beginning training. I had previously certified in a “Billings-based method” but learned quickly that authentic Billings is a different creature altogether.
I recommend that anyone who is going to train in this method learn to practice it first for at least 6 to 12 cycles under the guidance of an accredited teacher. Joining this program without learning the method first is going to leave you lost on your charts – when you should be confident in your charts before helping others.
Second Step:
The class began in December 2019 and ran through September 2020. We met once a month for approximately an hour (sometimes a little more or less). Inbetween meetings, we were expected to read one to two chapters of material and complete 5 or more worksheets that included chart evaluation and quizzes.
I really appreciated the live classes because my previous certification had no live component. I’m a strong believer that synchronous connection is really important for learning something new.
During class, we were shown PowerPoints and given time to ask questions about the homework. Hearing from long-term accredited teachers about different charting circumstances did wonders for my existing knowledge base. It was incredibly valuable.
Full disclosure: It is important to know that Billings was founded by and is primarily run by Catholics. These meetings often began with prayer or referenced God. Teachers are not required to teach the religious component of the PowerPoint. That means that Billings can be presented in a secular manner. The WOOMB International head organization notably does not include religious elements in their presentation of the method. The science of the method is solid regardless of any ideology attached to it.
Third Step:
The next step after passing an exam on the material was to begin practicum. Practicum is the supervised portion of the certification where you teach 6 to 10 clients minimum in the method while submitting charts and questios to a supervisor selected for you by the organization.
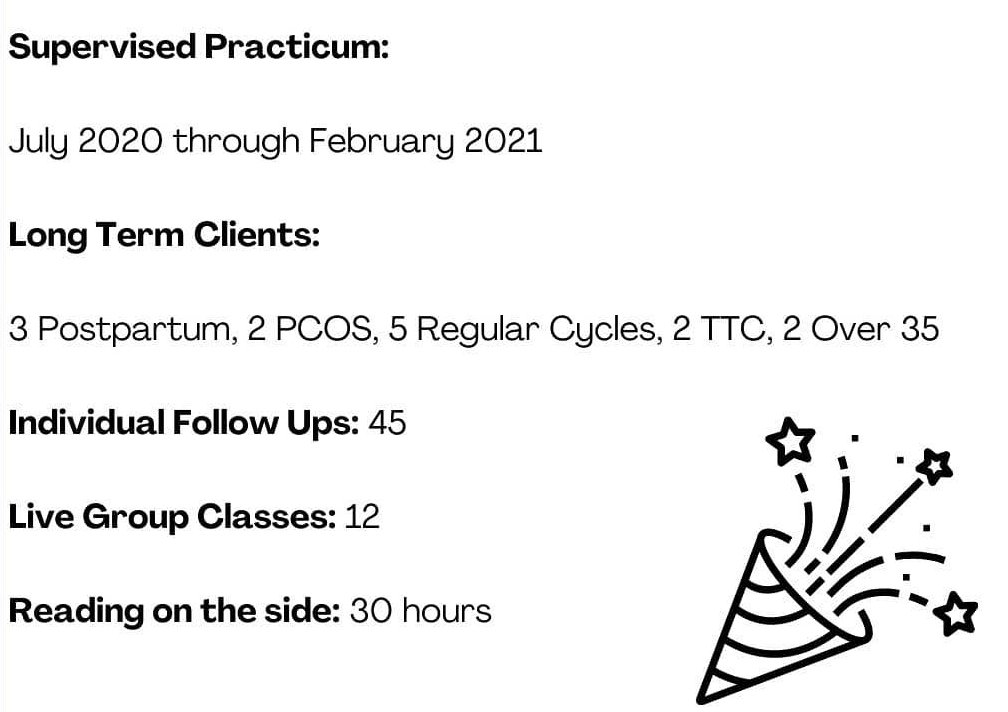
Practicum was the most enriching part of the experience, and I recommend that anyone who does the training utilize this time to your best advantage. I learned how to help people identify complex basic infertile patterns where they never have dry days. This was not possible in my previous method. I was able to support multiple postpartum women as well as folks with PCOS or who were trying to conceive. I learned so much by meeting with my clients and sending charts to my supervisor.
The follow-ups and classes in Billings are mandatory live meetings (video calling, phone call, or in-person). The follow-ups generally last 15 to 30 minutes depending on the client and how early they are in the process. Follow-ups and classes are required to be live, and this is based on what was done to reach efficacy in the Billings studies. We generally meet with clients seven or more times in the first 6 months, and then every 1 to 3 months. Some people may have more or less follow-ups depending on when they reach autonomy and things like cycle characteristics (postpartum people tend to meet up until the third ovulatory cycle after return of fertility.)
Fourth step:
After having enough clients in different situations (postpartum, trying to conceive, trying to avoid, regular and irregular cycles), I had a final meeting with my supervisor. Before this, I had to compile a document of every client chart. This was a bit laborious as the Billings charts cannot be exported to PDF without losing part of the chart. I had to screenshot segments of the charts and then re-assemble them. This meeting with my supervisor lasted about two hours, and we discussed all of my client charts and any corrections that needed to be made.
Following that, I was recommended for the final step. I recieved a mailed in exam that involved correcting a full paper chart and writing why I made those changes and what mistakes were originally made.
I turned in this exam to two graders. They then met with me and discussed the chart and any necessary corrections. They approved my certification at the end of the meeting.
The Future
Billings Ovulation Method teachers are required to do continuing education to maintain their certification. This is an investment of approximately $300 to $600 every three years. While this is costly, it is really important to attend further training where the teacher can see more advanced charting techniques and learn about health conditions, efficacy, and more!
My Final Thoughts
I would recommend this certification program to anyone who is interested in having an in-depth understanding of cervical mucus charting. The Billings Method teaches about things like the “pockets of shaw” and the cervical mucus crypts. My previous certification did not include close study of the patterns of cervical mucus. This program fundamentally changed my thinking about temperatures always being a necessary part of charting. I ended up dropping temperatures completely after 3 years of using basal body temperature.
Billings allows teachers to order all supplies, including digital materials, for clients. This means I do not have to produce my own materials, and it is super useful for quickly mailing clients what they need.
To make the most of out of this program, I recommend also reading the scientific studies on the side. Unfortunately, the program did not go into a lot of depth on the previous research studies. As someone in academia, I really like understanding all the different correct use and typical use statistics. I’m often questioned about efficacy, and I want to be able to answer people’s questions. If this also describes you, I recommend the following articles:
The Discovery of the Different Types of Cervical Mucus
Use-effectiveness and client satisfaction in six centers teaching the Billings Ovulation Method.
Field trial of billings ovulation method of natural family planning.
A prospective multicentre trial of the ovulation method of natural family planning
A Trial of the Ovulation Method of Family Planning In Tonga
A Response: In Defense of Truth in the Science of the Billings Ovulation Method











































You must be logged in to post a comment.